Get in Touch with Tongren Tang Gulf
💡 Shoulder Pain at a Glance
| 12-month prevalence | Median 16% of adults |
| Annual incidence | 7.7–62 per 1,000 person-years |
| Women vs. men | 20.2% vs. 12.5% |
| Most common cause | Rotator cuff conditions |
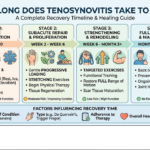
| Typical recovery | 2–12 weeks (conservative), 3–6 months (surgical) |
What Causes Shoulder Pain? The Most Common Conditions Explained

Approximately one in six adults experience shoulder pain annually, as noted by a 2022 systematic review in BMC Musculoskeletal Disorders. As the most mobile joint in the human body, our shoulder joint’s extreme range of motion results in reduced stability. Knowing the common causes — and when they demand professional attention — is the first step toward recovery.
Rotator Cuff Tears and Tendinitis
The rotator cuff comprises four muscles and their tendons that provide articulation stability to the head of the humerus within the shallow shoulder socket of the scapula. Among those younger than 60, rotator cuff tendinitis stands as the most common etiology of shoulder pain caused by overuse in reaching above head height. Partial- or full-thickness rotator cuff tears are more common with advancing age; studies reviewing imaging of asymptomatic shoulders found tears in over 30% of 65- to 70-year-olds. Classic complaints include pain at the lateral or anterior shoulder that exacerbates on overhead reaching or hand-tucking behind the back.
Frozen Shoulder (Adhesive Capsulitis)
Adhesive capsulitis (frozen shoulder) involves progressive stiffening and inflammation of the capsule surrounding the shoulder joint, resulting in loss of range of motion. It afflicts between 2% and 5% of the general population; the incidence increases 13-fold among diabetic people, with 17% of diabetics experiencing the ailment. According to a meta-analysis in the Journal of Diabetes Investigation, those with an A1c level exceeding 8% demonstrated the highest burden of frozen shoulder, with a 21.11% prevalence. The ailment has three stages of variable duration, namely freezing, frozen, and thawing, and usually lasts from 12 to 36 months.
Shoulder Impingement and Bursitis
Shoulder impingement syndrome involves repetitive pinching of the rotator cuff tendons or subacromial bursa within the specific range of arm elevation between 60° and 120°. Resulting tenderness known as bursitis occurs within the midrange abduction movement arc, and clinicians note a characteristic painful arc. Reaching overhead is a common task among painters, housekeepers, carpenters, contractors, and the like.
Osteoarthritis and Referred Pain
Glenohumeral osteoarthritis manifests as dull, sometimes intense ache and loss of motion that latterly worsens with activity. Growing burden of the disease among elderly patients makes it one of the rising sources of shoulder pain among those older than 65. A counterintuitive trend of note is that while the prevalence of shoulder pain climbs between middle age and the early 60s, it drops in older adults, perhaps due to lifestyle adaptations, or altered sensory perception associated with aging. Referred pain from the cervical spine, shoulder socket instability, or even cardiac events can mimic shoulder injuries, making accurate diagnosis essential.
| Condition | Typical Age | Key Symptom | Recovery Timeline |
|---|---|---|---|
| Rotator cuff tendinitis | 30–60 years | Pain with overhead reaching | 6–12 weeks (conservative) |
| Rotator cuff tear | 40+ years | Weakness + night pain | 3–6 months (post-surgery) |
| Frozen shoulder | 40–60 years | Progressive stiffness in all directions | 12–36 months (self-limiting) |
| Shoulder impingement | 25–50 years | Painful arc at 60°–120° abduction | 4–8 weeks (with PT) |
| Glenohumeral osteoarthritis | 60+ years | Deep ache + grinding on movement | Ongoing management; shoulder replacement if severe |
What you should remember: the rotator cuff makes up most of the reasons someone would get shoulder pain, however, the cause of shoulder pain depends upon the age, degree of activity and previous history of the individual. Getting a diagnosis is important for treatment.
Symptoms, Diagnosis, and When to See a Doctor

Understanding what’s causing your shoulder pain — where it hurts, when it’s worse, what helps or aggravates it — allows your doctor to pinpoint the problem and begin discussion about treatment options. Many sufferers put off getting help for shoulder problems, although some patterns of pain require urgent assessment.
Reading Your Symptoms
For the location of the pain to be a guide, it would be a very reliable one. Pain at the front, top or side of the arm is likely to indicate a shoulder problem- rotator cuff, impingement, bursitis. Pain below the elbow is more likely to be an issue with the cervical spine or nerve rather than the shoulder.
Night pain disturbing sleep is a marker for a rotator cuff tear and stiffening in the morning which later gives way for a while is common with frozen shoulder or arthritis.
Another often neglected factor is the thoracic spine. Mid-back stiffness can affect mechanics of the scapula and produce a situation that resembles and feels like a shoulder joint injury. If shoulder treatments produced no outcome after several weeks, a thoracic spine assessment may be the answer.
How Doctors Diagnose Shoulder Pain
The diagnosis still is based on a physical exam. Your doctor will assess your active and passive range of movement, specific muscle groups and doing tests where you are asked to reproduce the pain with certain maneuvers that can tell to which structure the pain is coming. In most of the cases the diagnosis is made clinically, according to the NHS guidance on shoulder pain.
Imaging is requested when an abnormality is suspected. Radiographs are necessary to exclude lesions such as fractures, osteophytes and arthritic changes. Ultrasound is being more commonly used as a first-line investigation for soft tissue integrity – ultrasound is inexpensive, and readily available and can diagnose rotator cuff tears in real time during movement.
MRI is the most detailed investigation and used mainly for surgical planning or if diagnosis remains uncertain after examination and ultrasound.
⚠️ Red Flags — See a Doctor Immediately If You Experience:
- Sudden, severe shoulder pain after an injury or fall (possible fracture or dislocation)
- Visible deformity of the arm or the complete inability to move the arm.
- A numb or tingly ‘electric shock’ sensation descending from the arm and into the hand.
- Chest pain or difficulty breathing with shoulder pain (Considering cardiac event)
- fever and swelling, redness or heat in shoulders (possible infection)
- Several cases of severe shoulder pain that continued for a period greater than two weeks without improvement.
These red flags can be a sign of shoulder dislocation, instability, or other conditions that require urgent medical care. Pain that persists beyond two weeks, disrupts your sleep consistently, or prevents you from performing daily tasks also justifies a medical evaluation — even without the dramatic red flags above.
Key takeaway: A careful physical exam often tells more than an MRI. But if your pain is sudden, severe, accompanied by numbness, or simply not improving, do not wait — get professional assessment.
Medical Treatments for Shoulder Pain: What Works and What to Expect

Shoulder pain treatment has shifted significantly in 2025. The American Academy of Orthopaedic Surgeons’ (AAOS) 2025 Clinical Practice Guidelines on the management of shoulder osteoarthritis and rotator cuff tear now offer stronger, evidence ranked guidelines on the management of rotator cuff tears – and several of those guidelines are counter to habits developed over decades of rotator cuff treatment. Here is what the evidence says about how to treat shoulder pain effectively.
Physical Therapy: The First-Line Treatment
Standard for virtually all shoulder conditions (except glenohumeral arthritis) – patients should first undergo a formal physical therapy program. This typically takes the patient through pain control/low-mobility work, rotator cuff and scapular strengthening, and sport- or task-specific training. Duration will usually be 6-12 weeks, two to three times a week.
Expected that patients will receive home exercises in addition to physical therapy – what is interesting is that the 2025 AAOS Clinical Practice Guideline indicated that patients could have similar benefits with home exercises without therapy. This was most evident in treatment of small rotator cuff tears. Does not discount the physical therapist, but this does prove that the home strengthening exercises are why the patient improves, not necessarily the therapist guiding them in office.
Injections: New Limits on Corticosteroids
📐 Engineering Note
The 2025 AAOS Clinical Practice Guidelines recommend placing only one corticosteroid injection with local anesthetic in the subacromial space or glenohumeral joint. Isolated cortisone injections will no longer be used to treat shoulder pain – repeated injections affect tissue strength in the rotator cuff, and would greatly increase infections if surgery is necessary. Source: AAOS 2025 CPG, 14 strong + 7 moderate recommendations.
Prior to the 2025 guidelines, many providers would give 3 or 4 steroid injections over multiple months if the patient was not improving. Updated AAOS guidance brings this practice to a halt. The guideline writers recognized that a single injection can have significant effect on pain and provide the physical therapist a window to treat, but NO additional injections should be given for fear of weakening the tissue for potential surgery later.
Evidence surrounding injections of platelet-rich plasma (PRP) remains inconclusive or only moderately beneficial. For partial rotator cuff tears, some studies have demonstrated benefit, but for pain relief in the short term, many studies find no statistically significant advantage over cortisone injections.
Surgical Options
Shoulder surgery in most cases is performed after 3-6 months of failed conservative therapies, or in the case of traumatic tears in younger/active patients. Two major updates in post-operative care are included in the 2025 AAOS guidelines: the patient can toss the sling in the closet for daily tasks at time 0, and the use of bioinductive (growth) implants received a Top Strong recommendation for rotator cuff repair adjuvants.
In cases of advanced glenohumeral osteoarthritis that is not improving with non-operative management, shoulder replacement procedures are an option. In cases of irreparable rotator cuff tear without adequate soft tissue coverage, reverse total shoulder replacement has increased significantly as a reliable option.
| Method | Best For | Timeline | Evidence Level |
|---|---|---|---|
| Physical therapy / home exercises | Impingement, small rotator cuff tears, frozen shoulder | 6–12 weeks | Strong (AAOS 2025) |
| Single corticosteroid injection | Acute pain flare, bursitis | Relief in 3–7 days; lasts 4–12 weeks | Strong — single injection only (AAOS 2025) |
| Arthroscopic rotator cuff repair | Full-thickness tears, failed conservative care | 3–6 months to functional recovery | Strong (AAOS 2025) |
| Bioinductive implant augmentation | Adjunct to surgical repair | Integrated into surgical recovery timeline | Strong recommendation (AAOS 2025, new) |
| Shoulder replacement | End-stage arthritis, massive irreparable tears | 6–12 months full recovery | Well-established; strong registry data |
Prognosis for recovery varies depending on severity of disease. Mild shoulder overuse related pain may resolve in 2 to 8 weeks with rest coupled with exercises tailored to correct common imbalances. Rotator cuff tendinitis is typical observed resolution is 6 to 12 weeks. After rotator cuff repair surgery time for full recovery and return to activity is typically 3 to 6 months per the AAOS OrthoInfo conditioning guidelines.
💡 Pro Tip
Inquire directly about the 2025 AAOS guidelines if multiple cortisone injections are suggested to you by your physician. Now overwhelming evidence exists in favor of one injection; this knowledge affords you a more informed discussion regarding how to proceed with your shoulder pain.
Traditional Chinese Medicine for Shoulder Pain: Evidence and Methods

Support for traditional Chinese Medicine (TCM) approaches to shoulder pain from clinical research continues to develop at a steady rate. The emerging picture is complex although certain trends are becoming clearer. Here is a summary of what the research actually shows.
Acupuncture: Where the Research Stands
Acupuncture has the most clinical evidence behind it for musculoskeletal pain. A randomized controlled trial involving 424 patients demonstrated that 65% of those receiving acupuncture for shoulder pain described clinically significant improvement at 6 weeks versus 24% treated with sham acupuncture, a significant difference in outcomes. This 2009 study published in the Annals of Internal Medicine remains the largest acupuncture study conducted on shoulder problems.
Support of TCM modalities other than acupuncture is mixed and less well documented. A Cochrane systematic review on acupuncture for shoulder pain supports its medium term efficacy but not its early results. Overall, acupuncture appears to work time-delayed rather than time-locked and that measurable effects often accumulate over the course of treatment.
The most interesting aspect of the available research is how widespread use has become of many modalities in the international guidelines. A 2024 review in BMC Complementary Medicine documented that 40% of guidelines addressing acupuncture relative to other conditions also reference shoulder pain and frozen shoulder. Combined acupuncture plus ongoing rehabilitation research provides moderate certainty evidence of significant short term pain reduction and gains in function.
Tui Na, Cupping, and Herbal Medicine
Tui Na (Chinese therapeutic massage) focuses on specific acupoints and select meridians with surface manipulation comprising pressing, rubbing, and stretching. For shoulder pain or stiff joints, the goal is to break overlying adhesions between the joint itself and muscles of the shoulder girdle. Restoring blood flow to the impacted areas is a secondary benefit. Such studies as exist have small subject populations whose results consistently show high patient ratings and no adverse events.
Cupping therapy (dry and wet) has evidence for myofascial shoulder pain. A systematic review published in 2022 in a Wiley journal found moderate evidence for pain relief and functional improvement in myofascial pain syndromes which included myofascial shoulder pain; the authors noted the included studies were highly variable in quality. Moxibustion (the application of heat produced by burning mugwort on or near acupuncture points) is frequently combined with acupuncture for “cold type” shoulder pain that increases in cold and humid weather. Safety data for all modalities demonstrated occurrence of adverse events were uncommon, most minor (ecchymosis, skin irritation) and of short duration (1-7 days).
The TCM Diagnostic Framework
Few shoulder pain patients respond to a purely Western medicine approach, may benefit from Eastern medicine TCM diagnostics, and find TCM therapies effective through self-help techniques. In TCM theory, most shoulder pain fits into the “Bi syndrome” pattern of Wind Cold Damp invasion of the channels. While this sounds nonspecific to those used to Western anatomy and diagnoses, the purpose of the observed pattern diagnosis is for treatment. A pain that flares in cold and humid weather may need a different prescription of herbs and acupuncture points than one that is achy-hot, swollen and tender.
At Tong Ren Tang – founded in 1669 with over 350 years of clinical TCM heritage – our practitioners assimilate these traditional prescriptions with modern orthopedic knowledge. Should you choose an integrated approach, you can learn about shoulder pain treatment at Tong Ren Tang to see how acupuncture, Tui Na, and herbal medicine complement standard care.
The main point: among traditional Chinese medicine modalities, acupuncture trials have the most convincing evidence for shoulder pain, and the results come on gradually over 4-6 weeks. The honest story: it is more effective than placebo, but it is not a cure for a shoulder with a complex structural problem like a large rotator cuff tear; it is only one part of a larger toolbox.
Home Remedies and Exercises to Relieve Shoulder Pain

Many mild shoulder pain cases can be treated effectively with simple home exercises and remedies for shoulder pain without a clinic visit. But first: you must know which exercises to do, when should I use ice versus heat, and – just as important – When do I call a doctor? These recommendations are based on the AAOS rotator cuff conditioning program and recent physiotherapy evidence.
Six Exercises to Relieve Shoulder Pain
Home exercise program. Do these exercises daily and move on to strengthening once pain has resolved. Perform all exercises slowly and smoothly, without pain. If any exercise causes pain in the shoulder, adjust the position and technique or skip for now.
✔ Daily Exercise Checklist
1. Pendulum Stretch — Lean forward, let your affected arm hang. Swing in small circles, 10 circles each direction. 2× per day. Gradually increase circle diameter as pain allows.
2. Cross-Body Stretch — Pull your affected arm across your chest using the opposite hand. Hold 30 seconds, 3 reps each arm. You should feel a stretch at the back of the shoulder blade, not sharp pain.
3. Doorway Stretch — Stand in a doorway with your arm at 90°, forearm on the frame. Step forward gently until you feel a stretch across the front of the shoulder. Hold 30 seconds, 3 reps. This restores flexibility of the shoulder capsule.
4. Shoulder Blade Squeeze — Sit or stand tall. Squeeze your shoulder blades together as if pinching a pencil between them. Hold 5 seconds, 10 reps, 3 sets. This corrects posture and strengthens the muscles between the shoulder blades.
5. External Rotation with Resistance Band — Keep your elbow at your side, bent 90°. Rotate your forearm outward against band resistance. 10 reps, 3 sets. This directly targets the rotator cuff’s external rotators — strengthening the muscles most commonly involved in shoulder injuries.
6. Wall Climb — Face a wall. Walk your fingers up the wall as high as you can reach without pain. Hold 5 seconds at top, slowly return. 10 reps, 2 sets. Tracks your range of motion progress over time.
💡 Pro Tip
The AAOS 2025 guidelines showed that rotator cuff tendinopathy patients get the same results from a home exercise program as from supervised physiotherapy – and the reason is commitment to the program. Set a phone reminder and stick to the program for at least 6 weeks before reassessing.
Home Remedies: Ice, Heat, and Over-the-Counter Relief
When you get a new injury, the first step should be RICE (Rest, Ice, Compression, Elevation). Place an ice pack wrapped in a towel on the shoulder for 15-20 minutes every 2-3 hours for the first 2-3 days after the injury or pain flare. Ice causes blood vessels to constrict, which reduces edema, swelling, and pain.
Once past the acute phase, put heat on your shoulder before exercise. Using a warm towel or heating pad for 10-15 minutes increases the blood flow and prepares the joint to be stretched. A lot of people find alternating heat and ice to be effective for long term problems- heat before the exercise, ice after.
Regular, over- the- counter, NSAIDS (ibuprofen or naproxen) can be taken to help relieve pain and inflammation. They should be taken in the smallest dose possible, for the shortest amount of time. Topical NSAIDs (gels or patches applied directly to the shoulder) target the local area, thereby helping to limit systemic side effects.
Sleeping position too. If one shoulder is sore sleep on the other side, a pillow can be placed under the shoulder of the affected arm. If lying on your back, put a small pillow under the affected arm.
Do not lie with the arm overhead, this can aggravate impingement overnight by compressing the subacromial space.
⚠️ When NOT to Exercise
- Immediately after an acute injury with significant swelling
- Any exercise will produce a sharp and worsening pain (a dull stretch feeling is fine), then stop and rest.
- After shoulder surgery without explicit clearance from your surgeon
- If you experience numbness or tingling during the exercise
Preventing Shoulder Pain
Prevention involves four long-term habits that promote good shoulder health:
Posture and ergonomics if you work at a desk. Have your monitor at eye level, keep elbows close to torso and every 45 minutes take a 30 second shoulder roll break. Rounded-shoulder posture decreases the subacromial space.
Warmup muscles prior to coming in contact with them. Five minutes of arm circles, band pull-aparts, and small slow circles in the shoulder prior to sport or manual work serves to warm up the rotator cuff and make it less susceptible to injury. Muscle and tendons cold are several times more susceptible to injury.
Progressive loading. If you are lifting weights, taking up a new sport or returning from injury, no single progression should increase the load (intensity) by more than 10-15% per week. The rotator cuff tendons require time to adapt to new demands and rushing this adaptation is one of the most consistent factors in inducing shoulder pain.
Wakeup stretching (5 min). Swinging your arms back and forth, stretching across the body, and light squeezes of shoulder blades all morning long will keep your joint loose and save you from pain before it takes hold. An investment in your body that is more relevant after 40 years old when tendons are less elastic.
Major lesson learned: For most mild shoulder pain, every day at home and even basic solutions will solve most cases. If you can spend 6 weeks solidly doing them, that always beats intermittent irregular efforts.
FAQ — Shoulder Pain Treatment
Q: What is the fastest way to relieve shoulder pain?
View Answer
For instant alleviation, ice for 15-20 minutes and try an NSAID from the drug store such as the ibuprofen. Gentle pendulum exercises may help loosen up without stressing the joint. If the discomfort is debilitating or if there has been trauma, do not attempt the above remedies but seek medical attention – the doctor may order imaging to check for a fracture or significant tear before engaging in activity.
Q: How do I know if my shoulder pain is serious?
View Answer
Get medical attention if your pain is sudden onset following injury, you are unable to move the arm at all, or if you experience numbness radiating down to your hand. Shoulder pain with chest tightness or fever should also be investigated. Pain that progressively worsens over two weeks despite rest should be examined.
Q: Can shoulder pain go away on its own?
View Answer
Yes — many causes of mild shoulder pain following muscle strain or overuse settle with rest and simple home treatment in 2-4 weeks. even frozen shoulder settles by itself, though it can be as long as 1-3 years. pain should be assessed if persistent or worsening.
Q: What anti-inflammatory is best for shoulder pain?
View Answer
Ibuprofen and naproxen are the two most easily available OTC medications. Naproxen has a longer duration of effect per dose (12 hours as apposed to 6-8 hours); making it useful for over night relief. Topical application of NSAID gels directly to the shoulder can also be effective with reduced gastrointestinal side effects.
Always ask your doctor if usage is for longer than 10 days.
Q: How should I sleep with shoulder pain?
View Answer
Sleep on your unaffected side, with a pillow between the arms, keeping the painful shoulder in a neutral position. Sleeping on the unaffected side with a pillow between the arms will encourage sleeping on a natural position. Sleeper on the back with a small pillow or rolled towel beneath the affected arm for support.
Do not sleep on the affected side with the arm elevated. It compresses the subacromial space and may aggravate rotator cuff and impingement pain. For some people, sleeping on a recliner or a wedge pillow at an incline of 30-45 degrees can relieve shoulder pain at night.
Q: Does acupuncture work for shoulder pain?
View Answer
Is there any evidence?
Evidence is variable; a recent large scale RCT of 424 comparing acupuncture alone to sham where 65% versus 24% responded at 6 weeks. The Cochrane reviews suggest that differences 2-4 weeks may be less obvious. Acupuncture seems to have the best outcomes when used as an adjunct with exercise therapy or in the form of a course of 4 to 8 sessions rather than a single application (huge placebo response).
Rare side effects have been noted such as potential bruising.
Q: When does shoulder pain require surgery?
View Answer
Operative repair should be considered after failed conservative trial of 3 to 6 months of physical therapy. Acute full-thickness rotator cuff injuries and irreducible unstable dislocations may warrant earlier surgical intervention.
Ready to Address Your Shoulder Pain?
Dealing with a chronic shoulder problem and require a solution that takes into account ancient wisdom and modern evidence? Tong Ren Tang in the UAE provides acupuncture, Tui Na, herbal medicine and cupping solutions suited to your condition – drawing from a clinical heritage of over 350 years.
About This Guide
This shoulder pain management guide was created by clinicians at Tong Ren Tang with over 350 years of traditional Chinese medicine knowledge combined with studies from modern Orthopedics such as the 2025 AAOS guidelines. We provide both standard Western treatments and traditional Chinese medicine methods transparently – including where evidence has been proven as well as where further investigation is required – because informed patients can make good treatment options.
References & Sources
- PMC9730650 — Systematic review of shoulder pain prevalence (BMC Musculoskeletal Disorders, 2022)
- PMC4915459 — Adhesive capsulitis and diabetes: meta-analysis (Journal of Diabetes Investigation, 2016)
- AAOS 2025 Clinical Practice Guideline — Management of Rotator Cuff Injuries
- AAOS OrthoInfo — Rotator Cuff and Shoulder Conditioning Program
- PubMed 19489707 — Acupuncture for chronic shoulder pain: RCT (Annals of Internal Medicine, 2009)
- Cochrane Library — Acupuncture for shoulder pain (systematic review)
- PMC12403485 — Clinical practice guidelines addressing acupuncture (BMC Complementary Medicine, 2024)
- NHS.uk — Shoulder pain: symptoms and when to get help