Get in Touch with Tongren Tang Gulf

Quick Specs
| Arthritis Types Covered | 5 (OA, RA, Gout, PsA, AS) |
| Treatment Categories | 4 (Medical, Complementary, Self-management, Integrative) |
| Evidence Sources | WHO, CDC, ACR, PMC meta-analyses |
| Reading Time | ~10 minutes |
| Last Updated | April 2026 |
What Is Arthritis — And Why Does It Affect Over 350 Million People?

Arthritis is a broad term covering more than 100 conditions that affect the joints and surrounding tissues. These conditions cause joint pain, swelling and stiffness around the joints and nearby tissue. Some types damage cartilage gradually over decades. Others activate the immune system attack on healthy tissue of the joint lining over months.
According to the CDC 58.5 million adults in the US- about 21.3% of the adult population- were diagnosed with some form of arthritis. Females are affected at a much higher rate (21.5%) than their male counterparts (16.1%).
Worldwide, osteoarthritis alone was estimated to affect 595 million people in 2020, which is a 132.2% increase from 1990. This rate does not seem to be slowing down as the global population ages and obesity increases.
Five common types of arthritis — including post-traumatic arthritis from prior injury — follow different pathophysiologic mechanisms. Each type requires its own approach, and the medications used to treat one form may not help with pain caused by another:
| Type | Mechanism | Common Joints | Typical Onset | Key Marker |
|---|---|---|---|---|
| Osteoarthritis (OA) | Cartilage degeneration (wear-and-tear) | Knees, hips, hands, spine | Age 50+ | Joint space narrowing on X-ray |
| Rheumatoid Arthritis (RA) | Autoimmune — attacks synovial membrane | Hands, wrists, feet (symmetric) | Age 25–50 (women 3x more likely) | RF+, Anti-CCP antibodies |
| Gout | Uric acid crystal deposits in joints | Big toe, ankle, knee | Age 30–50 (men earlier) | Elevated serum urate |
| Psoriatic Arthritis (PsA) | Autoimmune — linked to psoriasis skin condition | Fingers, toes, spine, entheses | Age 30–55 | Dactylitis (sausage digits) |
| Ankylosing Spondylitis (AS) | Chronic spinal inflammation | Sacroiliac joints, spine | Age 17–35 (men 2–3x) | HLA-B27 positive |
Knowing which type of arthritis you have is the first and most important step in optimizing your treatment plan. A rheumatologist can distinguish between each of these conditions with laboratory tests, imaging of the affected joints, and physical examination.
Early Warning Signs — How to Recognize Arthritis Symptoms Before Joint Damage Starts

Arthritis usually does not come on in a sudden and noticeable way (except gout). It tends to develop slowly over time, and catching early signs helps reduce long-term joint destruction and improve outcome. Current treatment modalities can halt the progression of many forms if started early enough.
Red flags by type:
- OA: Gradual joint pain and stiffness that is aggravated with activity and relieved with rest. Kerning in the knee and clicking in the hip when walking.
- RA: Symmetric swelling of small joints, especially in the fingers and toes. Joint stiffness for greater than 30 minutes in the mornings. Positive MCP/MTP squeeze test (Walking compressing and releasing causes pain).
- Gout: Rapid, disabling pain, especially in the big toe. Usually wakes people up at night. Swelling and redness peak in the first 12-24 hours.
When to see a specialist: When joint pain lasts longer than 4-6 weeks, if several affected joints have swelling, or if it is accompanied by fatigue and unexplained weight loss, your GP should refer you to a rheumatology center. Testing includes X-ray, MRI, ESR, CRP, RF, anti-CCP.
📐 Engineering Note: The Early Treatment Window
Research supported by the American College of Rheumatology shows that people who are treated within 3-6 months of inflammatory symptoms seek less aggressive therapies, have less joint destruction, less disability and achieve normal life expectancies. In RA the number of months delay directly correlates with the extent of joint destruction. The clinical window is real and it is short.
At what age does arthritis usually start?
It depends on the type. Various forms of arthritis appear at different ages. Osteoarthritis often occurs after age 50 but joint injuries can cause a damaged joint decades earlier. Rheumatoid arthritis usually presents 30-50, and females are three times more commonly affected. Gout usually affects men in their thirties. Juvenile idiopathic arthritis affects under 16.
I thought it was just aging- maybe I had slept in the wrong position or I had been overexerting myself at the gym. It took me 14 months to get seen by a rheumatologist. By then the erosion had already begun. – Patient forum phenomenon
Warning signs — see a doctor if you notice symptoms of arthritis such as:
- Morning stiffness that lasts more than 30 minutes—on rising, the synovitis causes pain and stiffness in the joints.
- Swelling of the same joint on both sides of your body
- Polyarthritis which persists for 4-6 weeks
- ✔ Unexplained fatigue paired with joint symptoms
- Sudden, severe inflammation and pain in a single joint (possible gout)
- ✔ Reduced range of motion that limits daily activities
Use our arthritis self-assessment to appraise your symptoms and see if you need to consult a specialist.
Conventional Medical Treatments — From Pain Relief to Disease Control

Depending on the specific arthritis, various treatment options exist to manage pain, from over-the-counter pain medication to the newest biologic therapies that act on specific immune pathways. Your selection will be based on your diagnosis, disease activity and response to initial therapy:
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
Nonsteroidal anti-inflammatory drugs like ibuprofen, naproxen and celecoxib are still first-line options to relieve pain and suppress inflammatory activity for arthritis patients. They are effective – often with little lag time – but they have significant side effects with chronic use: A number of meta-analyses have revealed GI complications in up to 30% of chronic NSAID consumers, including ulcers and bleeding. Others have demonstrated a positive relation with cardiovascular risk for prolonged applications – especially with high doses.
DMARDs (Disease-Modifying Anti-Rheumatic Drugs)
Disease-modifying antirheumatic drugs are the mainstay for inflammatory diseases such as RA and PsA. Methotrexate is the gold standard for treatment of RA, and the ACR 2022 guideline advocates a “treat-to-target” approach so that the dose is titrated until a preset low disease activity threshold is achieved. Initiating DMARDs within 3-6 months of RA can reduce pain and improve outcomes while delaying irreversible joint erosion.
Cost per year can be estimated between $500 and $2,000 for conventional DMARDs such as methotrexate and sulfasalazine.
Biologics and Targeted Therapies
When DMARDS alone cannot control the disease, biologic medication is the next step. These agents (the tumor necrosis factor (TNF) inhibitor ‘etanercept’ and ‘adalimumab’, the IL-6 receptor blocker ‘tocilizumab’, and the JAK inhibitors (‘tofacitinib’ and ‘baricitnib’) do not just shut down the immune system but attack the inflammatory cascade on specific and different levels. They work very effectively in moderate-severe RA, PsA and AS to get the disease under control – but at a cost: $39,000 to $55,000 per patient per year.
The development of biosimilars (such as Flixabi® and Yedali® in 2025-2026) is starting to bring the price down so more people can access targeted therapy.
Corticosteroid Injections
Intra-articular corticosteroid injection provides temporary relief by delivering medication directly into the affected joint — inflamed joints generally respond quickly (within 24–48 hours). The duration of response is limited (weeks to months) and multiple injections can hasten cartilage destruction. Typically most rheumatologists would restrict injections to 3–4 times a year per joint.
Joint Replacement Surgery
In end stage OA or severely destroyed joints through RA, patients who need surgery may benefit from hip and knee prosthetic replacement, which has been proven to offer the ultimate fix with success rates of over 90% of prosthetic joints functioning at 15 year follow up. Arthritis surgery is indicated at this stage when pain is uncontrollable with other conservative management options. In some smaller joints, joint fusion may be preferred over replacement.
📐 Engineering Note: DMARD Treatment Window
ACR recommends starting DMARDs within 3–6 months of RA diagnosis. Each month of delay results in a measurable increase in joint erosion scores. For RA patients, this window represents the single most important factor in long-term joint preservation.
There is a window of opportunity for intervention in RA to prevent joint destruction—namely, an early window.
– Theodore R. Fields, MD, FACP, Attending Physician,Hospital for Special Surgery
| Treatment | Mechanism | Onset | Duration | Key Side Effects | Annual Cost |
|---|---|---|---|---|---|
| NSAIDs | COX enzyme inhibition | Hours | 4–12 hours per dose | GI bleeding, CV risk | $100–$500 |
| DMARDs | Immune modulation | 4–12 weeks | Ongoing (daily/weekly) | Liver toxicity, infection risk | $500–$2,000 |
| Biologics | Targeted pathway blocking | 2–6 weeks | Ongoing (biweekly/monthly) | Serious infections, injection site | $39,000–$55,000 |
| Corticosteroid Injections | Local anti-inflammatory | 24–48 hours | Weeks to months | Cartilage thinning, blood sugar spike | $300–$1,500 |
| Joint Replacement | Prosthetic joint implant | 6–12 weeks recovery | 15+ years | Surgical risks, implant wear | $30,000–$50,000 (one-time) |
What’s the most effective treatment for arthritis?
There is no single answer. For RA, the best outcomes are achieved by combining DMARDs and biologics under a treat-to-target algorithm. For OA, physical therapy and specific exercises targeted to the joints outperform medications alone in many patients. For gout, urate-lowering therapies (allopurinol, febuxostat) prevent future flares once the serum urate is in the target range below 6 mg/dL.
“I learned the hard way that infections and biologics can be a dangerous mix. My rheumatologist had warned me, but I didn’t take it seriously until I ended up hospitalized with pneumonia. Now I get every vaccine on schedule and never skip my blood work.” –CreakyJoints patient community
Alternative and Complementary Approaches Backed by Research

Complementary therapies should not replace medical treatment in inflammatory arthritis – several are supported by sufficient clinical data to be considered as adjuncts. Here’s the evidence.
Acupuncture
Multiple 2025 meta-analyses confirm that acupuncture produces significant pain reduction for knee osteoarthritis. A review published in PMC found that: “acupuncture therapy shows significant advantages over the control group in reducing inflammation, reducing pain”.
A second systematic review of 2,056 subjects showed acupuncture to outperform sham acupuncture – eliminating the placebo effect – in treatment of OA pain. For those already using NSAIDs or DMARDs, the addition of acupuncture can be a potential way to reduce medication use.
Traditional Chinese Medicine (TCM) Herbal Formulas
In traditional Chinese medicine, arthritis is classified as a Bi Syndrome – a type of condition caused by wind, cold, dampness or heat ingress and obstruction of the meridians. Formulas such as Du Huo Ji Sheng Tang have been applied in the treatment of pain in the lower limbs for hundreds of years. A 2020 PMC review of combined traditional Chinese and conventional western medication in RA was encouraging, but the authors called for a need for larger scale studies and more treatment-specific protocols.
Physical Therapy and Exercise
The CDC recommends 150 minutes of moderate intensity, low impact weight bearing activity weekly for adults with arthritis. Swimming, cycling, yoga and tai chi have all demonstrated benefits for pain and improving joint range of motion. In particular, tai chi has been examined extensively for knee OA with measured improvements in physical health and psychological functioning.
Supplements
Glucosamine and chondroitin are some of the most common formulations taken over-the-counter. However, the ACR conditionally recommends against their use in OA, citing the often conflicting evidence. Omega-3 fatty acids (from fish oil or algae) have shown slight anti-inflammatory effects and should be used with the understanding that they are not a replacement for prescription medications.
Massage and Manual Therapy
Massage therapy can temporarily alleviate pain and improve joint range of motion. It should be thought of as a symptom management approach rather than a disease modifying intervention.
| Approach | Evidence Level | Best For | Limitations |
|---|---|---|---|
| Acupuncture | Strong (multiple meta-analyses) | Knee OA pain reduction | Less data for RA, AS |
| TCM Herbal Medicine | Moderate (integrated reviews) | RA adjunct therapy | Standardization challenges |
| Physical Therapy | Strong (CDC-endorsed) | All types, especially OA | Requires consistency |
| Glucosamine/Chondroitin | Weak (mixed results) | OA symptom relief | ACR recommends against for OA |
| Massage Therapy | Moderate (symptom relief) | Temporary pain management | Not disease-modifying |
If you are a patient in Dubai searching for herbal remedies and acupuncture for your arthritis condition, Tong Ren Tang offers a 7-month program combining 350 years of TCM wisdom with DHA-certified clinicians and acceptance from 7 major insurance carriers including AXA
See our detailed comparison of TCM vs conventional approach for one-page chart.
Daily Self-Management Strategies That Actually Reduce Arthritis Pain

There are many ways to manage arthritis and manage your symptoms beyond medication. Home remedies and daily habits help with pain and ease the pain of early arthritis flares. They cannot replace medical treatment, but every intervention works better when combined with consistent self-care that protects and strengthens the joints. And research continually supports this fact.
Anti-Inflammatory Diet
Observational studies link a Mediterranean diet pattern- high in fatty fish, olive oil, greens, berries and nuts- with antiinflammatory effects and lower inflammatory markers. Conversely, excess amounts of red meat, simple sugars and processed food worsen inflammation. Involves no severe restrictions. 6070% change in your intake of these antiinflammatory foods toward clean, whole foods, over a period of 812 weeks, can make a difference.
Weight Management
Your body weight directly increases the load on your joints. Every pound of weight lost takes off four pounds of stress from your knees according to the Arthritis Foundation. For a person who weigh 20 lb more than desired, that is four times that- 80 pounds with every single step.
Exercise
The Centers for Disease Control listed 5 core self-care approaches for arthritis including participation in 150 min a week of low-impact exercise. Water fluorishes because water peacefully supports your entire weight and adds resistance against body movements. For arthritis, walking, Recumbent Bike or Tai Chi are excellent starting options. Focus on duration rather than force on your joints.
Joint Protection and Ergonomics
Support braces, jar openers, grab bars lessen the load on your joints during daily activity. Cold packs are more effective for joints inflamed from activity while warm packs ease morning stiffness.
Stress and Sleep
Chronic cortisol elevations from ongoing stress culminate in increased inflammation. Pain from arthritis distresses sleep which in turn sharpens pain perception in a vicious circle. Deliberate attention to 78 hours a night of sleep, stress-relief strategies (mindful breathing, meditation, gentle stretches) breaks the cycle.
How do you stop arthritis from getting worse?
Early treatment combined with a strategic plan of 5 factors gets you through every single day: early diagnosis, healthy weight, low-impact activity, antiinflammatory eating habits and joint protection to prevent joint deterioration during daily activity. No single factor is enough but together they comprise the self- management fundamentals recommended by every rheumatologist.
“Your instinct says Not to move; to rest. And yes, rest is essential during a flare. But about a year ago, I began swimming 3 mornings each week and the pain and stiffness I experience is cut in half.” RA forum poster
“Ignoring gut health is one of the biggest mistakes arthritis patients make. Inflammation often begins in the gut and travels outward more than most realize.” — clinical practice observation
Pro Tip: Keep a journal of your symptoms, diet, exercise and sleep daily for 4 weeks. Patterns will emerge – and you’ll find your individual triggers faster than any blood test.
✔ Daily Self-Management Checklist
- . 30 minutes of low-impact activity (e.g., swimming, walking, tai chi)
- . 2+ servings anti-inflammatory foods (fish, greens, berries)
- . Morning hot pack (shower, heating pad) for stiffness relief (10-15 min)
- ✔ Joint protection during repetitive tasks
- ✔ 7–8 hours of sleep with consistent schedule
- ✔ 5 minutes of stress reduction (breathing, meditation, stretching)
How to Build Your Arthritis Treatment Plan — A Decision Framework
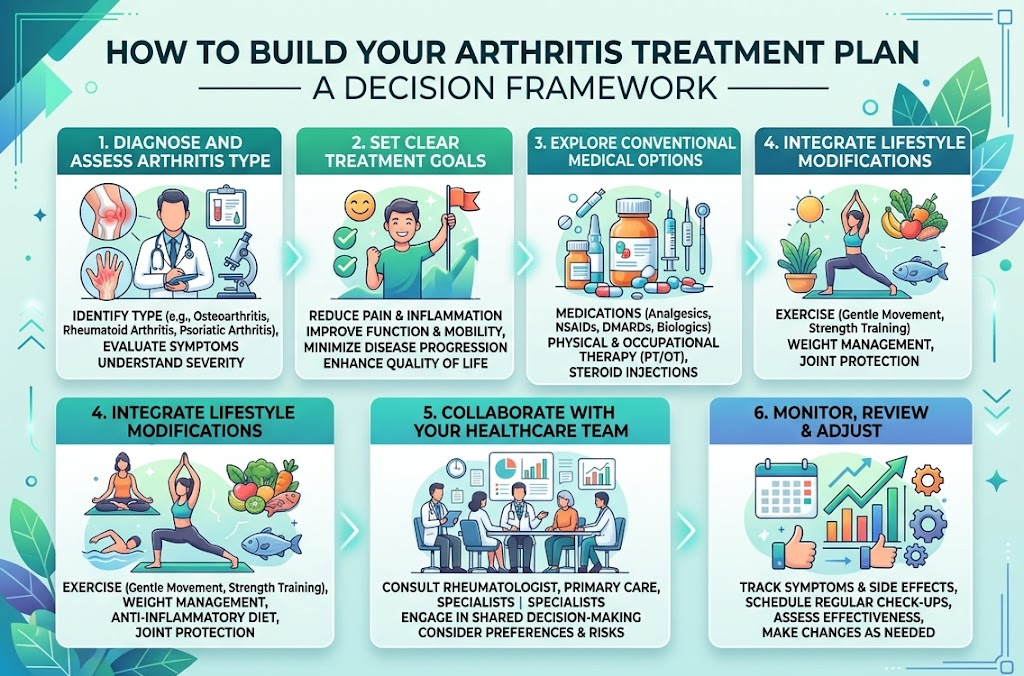
With so many effective therapies available, building a treatment plan that fits your condition prevents under- and over-treatment. The tiered framework below categorizes interventions by invasiveness, cost and strength of evidence to help you make your joints a priority.
The Treatment Ladder
Tier 1 — Self-Management Foundation
Anti-inflammatory diet + regular low-impact exercise + joint protection + weight management. Start here whether you have OA or an inflammatory type.
Tier 2 — First-Line Medical
NSAIDS (oral or topical) + physical therapy + topical capsaicin or menthol. Use when tier 1 is not effective enough for pain relief.
Tier 3 — Advanced Medical
DMARD’s + biologic agents + corticosteroid injections. Needed for inflammatory arthritis (RA, PsA, AS) and advanced OA that does not improve with tier 2.
Tier 4 — Integrative
Combine tier 2-3 approaches with evidence supported complementary therapies; acupuncture, Chinese herbal medicine, Tai chi and mind-body approaches. This tier focus on treating the whole person: pain, inflammation, function and quality of life.
| Severity | Recommended Starting Tier | Escalate If… |
|---|---|---|
| Mild | Tier 1 + Tier 2 as needed | Pain persists beyond 6 weeks |
| Moderate | Tier 2 + Tier 3 (if inflammatory) | Functional decline or joint erosion on imaging |
| Severe | Tier 3 + Tier 4 combination | Failure after 3–6 months of compliant treatment |
⚠️ 3 Red Flags to Escalate Immediately:
- Persistent pain for greater than 6 weeks despite current therapy.
- Morning stiffness exceeding 1 hour daily
- Visible joint deformity or sudden loss of range of motion.
For Dubai residents: Eleven major insurance carriers cover acupuncture when administered by authorized DHA practitioners. This allows integrative approaches at different tiers to be value accessible – verify your own insurance coverage before thinking it is outside of your budget.
Review the program or use our treatment cost calculator to determine your insurance-based out-of-pocket payments.
Frequently Asked Questions About Arthritis Treatment
What causes arthritis?
View Answer
Arthritis has various causes that differ by condition. OA is cartilage degeneration resulting from aging, injury or excess weight. Inflammation in RA/ PsA is immune-system-initiated attacking of joint tissue. Gout is caused by an excess of uric acid forming crystals in the joints. Each type has genetic, hormonal and environmental risk factors.
Can arthritis be cured permanently?
View Answer
There is currently no permanent cure for any type of arthritis. However, RA is often in consistent remission with early aggressive treatment with DMARD’s and biologics. Gout can be completely managed so there are no flares with uric-acid lowering therapies. OA can be dramatically slowed by exercise, weight management and joint protection. The focus of treatment is function remission: living pain free with no limitations.
Will arthritis get worse without treatment?
View Answer
The majority of patients benefit from fairly prompt treatment. If untreated, RA can lead to joint destruction and deformity in 2-5 years. -OA with joint space narrowing and potential bone-on-bone contact. Untreated gout progresses to tophi and kidney damage. Early intervention is the best predictor of positive long-term joint health.
What is the fastest way to relieve arthritis pain?
View Answer
For pain relief, a single dose of oral NSAIDs (ibuprofen, naproxen) clears up pain in just 1-2 hours. Corticosteroid injections while not always avoidable deliver instant relief (1-2 days) when injected directly into an inflamed joint. Topical NSAIDS available as gel (diclofenac) require less systemic absorption and travel more directly to the joint. Cold packs temporarily reduce swelling, heat is for morning stiffness. These intervention are often used on an as-needed basis;.
Does arthritis medication have side effects?
View Answer
Yes. Every arthritis medication has side effects. NSAIDS are liked to GI problems and cardiovascular risk with prolonged use.
Methotrexate and other DMARDs require monthly blood work to check liver function. It also blunts the immune system, which makes you more prone to infection. Your rheumatologist will do monthly blood work and then moderate medication doses compared to the risk.
Ready to Start Your Arthritis Treatment Plan?
Get a personalized treatment plan from DHA-licensed TCM practitioners at Tong Ren Tang Dubai. Accepted by 7 major insurers.
About This Guide
This article has been prepared by clinical content team at Tong Ren Tang Dubai using medically peer-reviewed evidence obtained from CDC, ACR, PMC, and Arthritis Foundation articles. Treatment recommendations are based on both scientific results of western medicine and Traditional Chinese Medicine data through clinical experience of last 350+ years. This guide is for educational purposes only and should not be treated as specific medical advice.
References & Sources
- CDC Arthritis Data Brief 2022 – cdc.gov
- PMC Global OA Prevalence Study (2020 data, 132.2% increase since 1990) — pmc.ncbi.nlm.nih.gov
- Recommended by the ACR 2022 guideline for the management of RA – rheumatology.org
- PMC 2025 Acupuncture Meta-Analysis for Knee OA — pmc.ncbi.nlm.nih.gov
- Arthritis Foundation Self-Management Resources — arthritis.org
- CDC Five Self-Care Strategies for Arthritis — cdc.gov
- HSS Early Diagnosis of Rheumatoid Arthritis – hss.edu
Related Articles
- Arthritis Treatment at Tong Ren Tang Dubai
- TCM vs Conventional Arthritis Treatment: A Side-by-Side Comparison
- Acupuncture in Dubai: How It Works and What to Expect
- The Anti-Inflammatory Diet: A Practical Guide for Joint Health
- Pain Management with Traditional Chinese Medicine
- Tai Chi for Arthritis: Evidence, Techniques, and Getting Started