Get in Touch with Tongren Tang Gulf
Medically reviewed by the Tong Ren Tang Gulf TCM clinical team · Last updated April 2026 · Evidence base: CHEST 2016 guideline, Mayo Clinic 2024, WHO Traditional Medicine Strategy 2025–2034, PMC12517813 (2024 review).
If you are on the hunt for honest answers on how to treat that common chronic cough you have probably exhausted all the usual suspects – cough drops, antihistamines, an empiric trial of reflux medication that flopped. A cough that has chipper overstay’s it’s welcome is no trifling matter, it is a clinical marker with a defined value, an evaluation algorithm and several treatment options that most patients won’t learn about until their second visit to their doctor.
Quick Specs: Chronic Cough at a Glance
- Definition: Adult cough for longer than 8 weeks, or in children for longer than 4weeks.
- Adult prevalence in developed countries: 10-20% of adults (per a 2024 PMC review)
- Top 3 in non-smokers: Upper airways cough syndrome (postnasal drip), asthma and gastroesophageal reflux disease up to 90% of cases3.
- Average diagnostic timeline: 8–12 weeks for cause-directed trial therapy
- Refractory or unexplained persistent cough rate: about 30% conform to typical refractory markers, with other definitions placing it between 1.5% and 60%
- First-line step : go through medication including ACE inhibitors – take full history and do an empiric treatment trial- no to a chest scan immediately.
What Is a Chronic Cough? The 8-Week Rule That Changes Everything

Clinical medicine makes a very fine distinction between the lingering bug and the chronic cough. For adults, the Cleveland Clinic, Mayo Clinic and the American Chest Physician Committee (CHEST) consider any cough lasting over eight weeks to be chronic and in children, four. Anything under three weeks is considered acute, three to eight weeks subacute, which being a self limiting condition, mostly resolves spontaneously.
Significance of this week is that it sets the course of diagnosis. In week two, whether a cough is anything more than a tail of infection depends on how long it lasts. By week nine, a cough is a Signifier for a hidden disease, however, it could also mean that the cough reflex itself has been hyper-sensitized and over responsive to stimuli that would normlly not provoke it, such as cold air or perfume.
Chronic cough rates in the developed world are estimated at anywhere between 10% and 20% of adult across all western countries and between 3.9% and 30% as per range of definition. It is one of the commonest presenting issues for adults attending a General practitioner consultation. However, the majority of patients seen in the clinic have experimented with two or three OTC remedies and waited for a while-a mundane cough until the eighth week passes and the story is quite different.
Coughing by itself is a normal protective reflex. Sensory nerves in the airway become activated when dust, mucus or acid irritates the upper airway or lung. For a chronic cough to remain, the reflex has either been triggered by a sustained stimulus– prolonged postnasal drip, silent acid reflux, airway inflammation– or the reflex itself has become hyperreactive.
Either way, waiting it out no longer helps past week eight.
Common Causes of Chronic Cough in Adults (The UACS–Asthma–GERD Triad + Rarer Drivers)
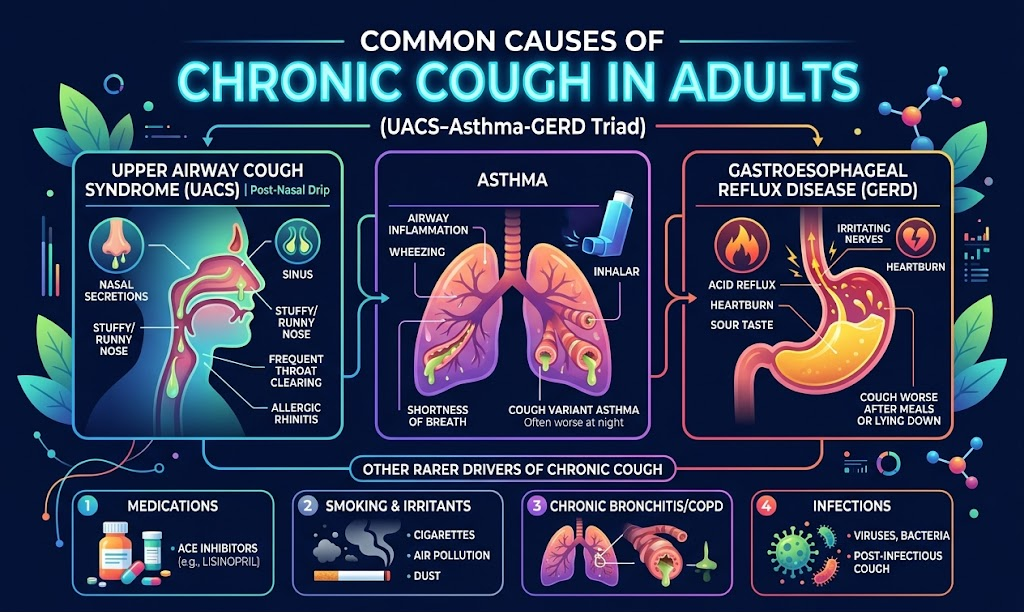
What Causes a Chronic Cough in Adults?
In non-smoking adults, these 3 entities account for 98% of all chronic cough. Quotes from prospective clinical trials cited in PMC6966942 show up to 90% chance of identification of the responsible path in a non-smoker by just these three, in combination or in series: upper airway cough syndrome, asthma, gastroesophageal reflux disease. This is the logical operational perspective: address the triad first, then seek other reasons once common causes have been exhaustively investigated.
Upper Airway Cough Syndrome (Postnasal Drip)
A nasal or sinus infection, allergy, or other nasal inflammation can cause excess mucus production which drips down the back of the throat and stimulates cough receptors. Signs include frequently clearing one’s throat, the sensation of mucus running down the back of the throat, or cough that worsens when lying supine. First step medication: antihistamines and nasal corticosteroid spray daily for 4-6 weeks.
Asthma and Cough-Variant Asthma
Cleveland Clinic’s clinical review identifies asthma as the commonest disease process to induce a cough amongst its patient population. This particular presentation, cough-variant asthma, may be missed for years as the only symptom is the cough (no wheeze, no shortness of breath). There is often a “cold air” factor triggering the cough as well as exercise or morning timing. Diagnosis is made with methacholine inhalation challenge testing. A 16-year diagnostic delay case in PMC4369981 illustrates how easy it is to miss.
Gastroesophageal Reflux Disease (GERD)
Your stomach may push acid back into the esophagus or, with silent reflux, into the larynx, to stimulate the cough reflex. Heartburn signs are surprisingly uncommon. An empiric trial of a proton pump inhibitor for 8 weeks is the typical treatment course. If other digestive complaints coexist, a separate digestive pattern evaluation may be appropriate.
ACE Inhibitor–Induced Cough
Starting ACE inhibition for B.P. – lisinopril, ramipril, enalapril etc. – can cause a cough as a side effect in 10% of patients. Symptoms begin weeks to months after initiation and resolve in 1-4 weeks after discontinuation and substitution with an angiotensin-receptor antagonist. Full medication history review with your doctor will clarify what’s causing the cough.
COPD, Chronic Bronchitis, and Less Common Causes
Among smokers and former smokers, COPD and chronic bronchitis are the dominant drivers of persistent cough. There are less common entities like eosinophilic bronchitis, bronchiectasis, interstitial lung disease and, feared by every patient with newfound cough, lung cancer. Lung cancer is a minority reason overall in chronic cough, yet a new persistent cough in a long term smoker or a cough with hemoptysis requires an urgent chest film. Allergy-driven respiratory inflammation can mimic or overlap with cough syndromes and must be given equal priority in evaluation.
“The practical rule is simple: in a non-smoker taking no ACE inhibitor, with a normal chest X-ray, run the triad sequentially – UACS first, asthma second, reflux third. About nine out of ten patients will get their answer in this loop.”
Cough Symptoms That Signal Red Flags — When to Seek Urgent Medical Care

Most chronic coughs are benign in origin. A handful aren’t. Certain associated signs and symptoms move the reading from “proceed through the work-up” to “we must see him this week or today.” This table groups cough signs and symptoms by rate of urgent finding – this is the red-flag triage most pulmonologists employ at triage.
| Symptom alongside cough | Urgency | Concerns to rule out |
|---|---|---|
| Coughing up blood (hemoptysis) | Same day / ED | Lung cancer, pulmonary embolism, tuberculosis, bronchiectasis |
| Unexplained weight loss >5 kg | Same week | Malignancy, tuberculosis, chronic infection |
| Drenching night sweats | Same week | Tuberculosis, lymphoma, endocarditis |
| Progressive shortness of breath at rest | Same day | Heart failure, interstitial lung disease, pleural effusion |
| Trouble swallowing or persistent hoarseness | Within 1 week | Head-and-neck cancer, laryngeal pathology |
| Broken ribs from coughing | Within 2 weeks | Severe cough intensity — needs targeted suppression plus cause workup |
None of these signs and symptoms in and of themselves mean that the worst case diagnoses (malignancy, TB, etc) is present. Rather they are the sign the workup should commence today, not after the cow has been dosed with every antihistamine in stock. If any of the above rows sound like your situation, schedule an appointment with the mouth and lung doc in person before reading further.
💡 Download the printable Red Flag Symptom Checklist
Keep it on your fridge or in your phone for a quick self-triage of urgency.
How Doctors Diagnose Chronic Cough — The Evaluation Pathway

Establishing a diagnosis of a chronic cough is often an exercise of positive and negative empiric treatment trials. There is no one pathology testing from which a diagnosis can be extrapolated. Instead, an experienced clinician guides a patient through 5 pathways, systematically excluding diagnoses by achievement in the pathway and genre. Pacing through the pathways matters: a rushed to CT-first visit is either very costly or provides little value for most patients with chronic cough, while a missed opportunity to review medications in depth can leave an ACE-cough untreated for decades.
What Tests Are Done for Chronic Cough?
Five stages most pulmonologists follow:
- Stage 1: History and physical. When was cough onset? Recent respiratory infection? Associated post-meal cough, nasal symptoms, or heartburn? Active or passive cigarette smoke, other inhalants in the office or home? Physical exam includes finger-bird examination of oropharynx, palpation of cervical nodes, and auscultation of the chest.
- Stage 2: Medications. Complete list of current prescriptions, with particular regard to you and all other blood pressure medicines. Swap out any ACE inhibitor for angiotensin receptor blocker for four weeks to watch for resolution of cough–a cheap, simple, indication than rule-out test.
- Stage 3: Empiric trial of therapy. For the most likely cause of the triad symptom cluster, a time limited trial: four weeks of antihistamines plus nasal steroid spray in response to suspicion for UACS, or eight weeks of omeprazole or equivalent in response to suspicion for GERD, or inhaled corticosteroid for two to four weeks in response to suspicion for asthma. Response to trial is itself proof if suspicion was correct.
- Stage 4: Spirometry with methacholine challenge. Lung function tests that identify asthma or cough-variant asthma when symptomatology does not include wheezing. Standard of care 4-8 weeks after initiation of empiric therapy trials if the cough fails to resolve.
- Stage 5: a CXR, a CT, bronchoscopy, rhinoscopy, or referral. CXR or a CT scan, bronchoscopy or rhinoscopy, or referral out to the bigs-withs at the cough clinics. Symptoms that never resolve despite work-up to this point or those that have a red-flag set of signs and symptoms prior to chronic cough prompting early airway endoscope or CT.
Patient reported symptoms are equally instructive. An NPR story in 2024 related the tale of a patient, Julie Silverman, who saw numerous providers before someone recognized the pattern. Such a patient experience is not an outlier – persistence, a detailed symptom log, and doing-the-suggestion to their best ability, follow-up visits with more intense adherence to empiric care all statistically improve the odds of a diagnosis.
Evidence-Based Treatment Options for Chronic Cough

There is truly not “a best treatment” for a chronic cough–the proper treatment depends on what the etiologic agent is. Our decision matrix below summarizes the first-line treatment lines for the major specific etiologic agents, based on the CHEST 2016 guideline and congruent with Mayo Clinic and Cleveland Clinic treatment modules.
| Cause | First-line treatment | Typical trial length | If no improvement |
|---|---|---|---|
| Upper Airway Cough Syndrome | First-generation antihistamine + intranasal corticosteroid | 4–6 weeks | ENT referral, sinus imaging |
| Asthma / cough-variant asthma | Inhaled corticosteroid ± long-acting beta agonist | 4–8 weeks | Add leukotriene receptor antagonist, reassess |
| GERD (with or without heartburn) | Proton pump inhibitor + diet and head-of-bed elevation | 8 weeks | Add prokinetic, esophageal pH study |
| ACE inhibitor–induced | Switch to angiotensin-receptor blocker | 1–4 weeks | Cough is not drug-related; reopen workup |
| COPD / chronic bronchitis | Smoking cessation + bronchodilator ± inhaled corticosteroid | Ongoing | Pulmonary rehab, specialist referral |
| Refractory / unexplained | Neuromodulator (gabapentin or pregabalin) + behavioral cough suppression therapy | 8–12 weeks | Specialist chronic cough clinic, investigational options |
A Note on Over-the-Counter Cough Drops and Suppressants
Dextromethorphan, codeine, and guaifenesin containing agents treat the symptom, not the disease. According to literature summarized by Mayo Clinic, oft-used OTC cough agents do no better than placebo for many patients. Menthol containing cough drops can soothe irritated mucosa, but in a subgroup of people with cough hypersensitivity syndrome have been reported to be paradoxically worsened by menthol. Use medications for short-term symptom control, not long-term planning.
Neuromodulators and Behavioral Therapy for Refractory Cough
Gabapentin and pregabalin, drugs off-label for use in neuropathic pain, are used to suppress cough-reflex hypersensitivity. It takes weeks to respond, and both drugs have dose-depend ent adverse effects—increased somnolence, dizziness. Behavioral cough suppression therapy delivered by a speech-language pathologist shows modest but statistically significant symptom improvement in randomized trials cited by the expert panel reviewing this evidence at CHEST 2016.
When Conventional Treatment Fails — Refractory & Unexplained Chronic Cough
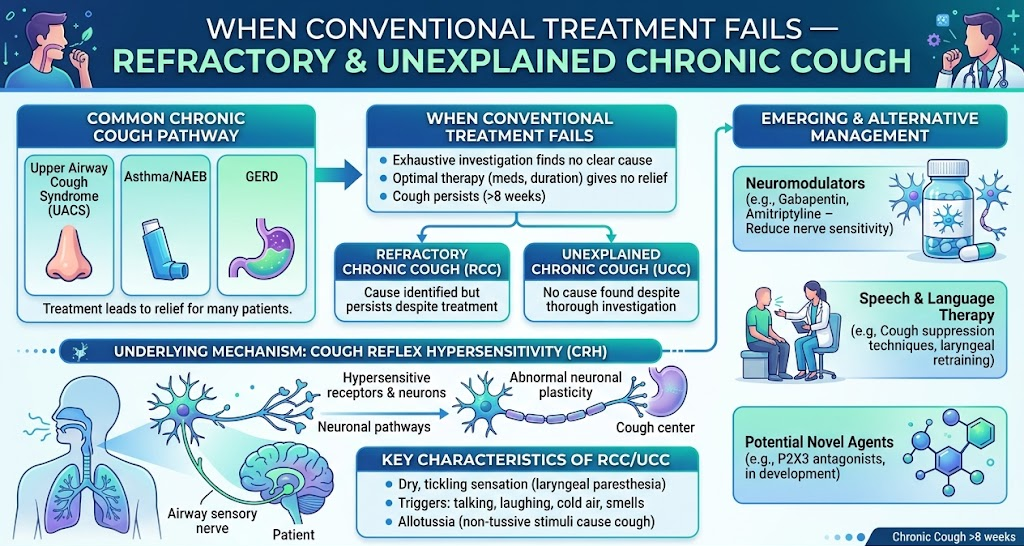
A minority of patients will run through the full diagnostic pathway, try every first line agents in correct dose and duration, and still cough. Here, the terminology is specific—refractory chronic cough having failed to respond to optimal treatment of the proven or suspected cause, versus unexplained chronic cough meaning the cause was not found despite investigation.
Why Up to 60% of Some Chronic Coughs Resist Treatment
Refractory numbers depend on how you count. One 2024 European Respiratory Journal Open Research study of 277 chronic cough patients put the rate at 30.7%, while a more strict case definition seen in another report would be zero like in our vignette, and a well-cited 2025 NEJM narrative review on adult cough reports that some reviews demonstrate “up to 60%”, though rigorous estimation is hard to come by. In practice, one-third of chronic cough patients will be unresponsive to guideline-concordant first- and second-line therapies, representing an important unmet need.
Emerging Options — P2X3 Receptor Antagonists
Gefapixant represents the first agent specifically developed for treatment of refractory chronic cough. It has not had an easy path through the regulatory process. In 2023 the FDA advisory committee recommended against its approval, and in the UK NICE terminated its appraisal. It is not yet available in the US or UK, but Japanese real world data provide some indication of benefit for selected individuals. Other P2X3 candidates are in development.
Traditional Chinese Medicine — A Pattern-Based Complementary Approach
For those patients with chronic cough not settling on conventional management, TCM is a worthy modality to become familiar with. While conventional medicine targets a pathological cough reflex arc, TCM seeks out its etiopathogenic functional pattern (whether cough occurs with clear phlegm, yellow phlegm, dry or sore throat, or sensation of heaviness in the chest) and provides a patent herbal prescription. The body of clinical evidence in favor of Traditional Chinese Medicine has been accumulating: the first GRADE-based Chinese herbal medicine cough practice guideline was published in 2023, a 2024 PLOS ONE scoping review indexing 474 traditional agent trials in chronic cough was published, and the acupuncture systematic review in PMC11815682 detailed that there were quantifiably fewer coughs passed during the observation period. By 2025, WHO’s Traditional Medicine Strategy (2025-2034) will officially endorse several traditional diagnostic models. For a pattern-based Chinese herbal medicine insight derived from 3 ½ centuries of clinical data, see the Tong Ren Tang TCM chronic cough treatment at Tong Ren Tang page, the Chinese herbal medicine principles summary and the glossary of TCM terms. Several adequate options exist for refractory cases that do not involve outdated and discredited concepts of expectorant or antitussive action, not as an alternative diagnostic approach to cause-directed medical approach.
Home Remedies and Lifestyle Strategies That Actually Help

Home therapies for chronic cough do not supplant dedicated etiology-based care, but they can lessen symptoms meaningfully as evidence of cause is investigated. The evidence tiers are transparently differentiated here in order to distinguish the sensible from the spurious.
Improved evidence: Inhalation of one teaspoon of honey at sleep time effectively soothes down irritant pathologies leading to cough and reduces overnight cough frequency in all patients aged over one year old, but never feed honey to infants less than 12 months old as that predisposes to the development of babybotulism. Adequate hydration (tap water, warm broths, herbal infusions) is a reasonable and cheap method of thinning gross mucus so it can be expectorated more readily. Enquire re sleep-disrupting nocturnal cough, and trial humidifier to add moisture in one’s bedroom.
Moderate evidence: Head elevation of the head-of-bed by 15-20 cm effectively reduces nocturnal reflux -related cough. Cessation of smoking is the simplest single intervention intervention for cough in smokers – expect a surge in cough as migration of airways clears in the first 7-14 days, then steady mitigation by 8-12 weeks. If one’s cough improves with gummi-vitis lozenges, then a sugarless commercial product containing glycerin is the best bet for evening dry throat (rather than menthol lozenges that threaten upper airway cachexia).
UAE- and Gulf-specific environmental factors: The PMC indoor air pollution review for the UAE discusses increased desert dust, shamaal wind, and dust-storms acting as asthma and cough triggers. Indoor air conditioning, while unavoidable, provokes airway irritation due to delivery of overly-chilled dry air. Incense and bakhoor odor, a ubiquitous presence in Arab houses, is a commonly-unknown cause of rich cough. Environmental interventions include the use of a HEPA-filter air purifier, maintaining indoor humidity at 40-50%, ventilating prior to and after odors-producing heat treatments, and matching internal air-con air filters with the OEM supplies until their clog up. Disturbed sleep from nocturnal cough — see the guide to sleep disruption linked to nocturnal cough — hinders complete convalescence
Top three chronic-cough home-remedy mistakes:
- Controlling a productive cough with OTC dextromethorphan– the cough is expelling mucous you need to be able to move.
- Abandoning an empiric trial of therapy at week two because nothing has changed– reflux and UACS trials often will need 6-8 weeks.
- Obscuring an ACE inhibiter on the medication list because it was started five years ago– ACE inhibitor cough can present months after initiation.
If you prefer a pattern-based self-assessment, the Tong Ren Tang service page hosts a five-question pattern-based TCM cough assessment that categorizes your symptom profile into one of four classical Chinese cough patterns.
Frequently Asked Questions
How long does it take for a chronic cough to go away?
View Answer
With a pinpointed diagnosis and targeted therapy, up to 93% of total coughs will resolve in 612 weeks, ‘UACS’ in 4-6 weeks following antihistamine plus nasal steroids, ‘asthma-related’ within 4-8 weeks following inhaled corticosteroids, ‘Gerd-related’ following eight weeks of proton pump inhibitors plus lifestyle measures, and more refractory coughs at the 8-12 week mark may require neuromodulators or behavioral therapy.
Why is my cough not going away after 2 months?
View Answer
If you find yourself at week eight or beyond on this chart your cough has become defined as ‘chronic,’ and the clinical approach is no longer ‘wait and see,’ but the search for a cause.
The most common explanation will involve an untouched participant from the Gerd-asthma-UACS triad or an ACE inhibitor medication side effect. Arrange to meet with a primary care or pulmonary specialist ask about empiric trial of therapy.
Is it normal to have a chronic cough?
View Answer
Common, yes -1 in 5 adults in developed countries will have a chronic cough at some point.
Normal?No. Any ‘cough that has lasted more than eight weeks’ merits investigation, in spite of the fact the eventual explanation may turn out to be benign.
Can Chinese medicine help with chronic cough?
View Answer
Experimental Chinese Medicine research into chronic cough has grown immensely.
A 2024 PLOS ONE scoping review indexed 474 clinical Chinese Medicine trials, a practice guideline has been written by the German states of Baden-Württemberg and Hessen based on the GRADE methodology, and systematic reviews have demonstrated statistically significant reductions in measured cough-frequency related to acupuncture. WHO’s 20252034 Traditional Medicine Strategy has assimilated Chinese Medicine diagnosis and therapy models. Chinese Medicine therapy is most effective when prescribed by a licensed practitioner who has completed pattern differentiation!-the Tong Ren Tang service page walks you through just one example.
What foods and environmental factors trigger chronic cough in Dubai?
View Answer
The Middle East region has known respiratory irritants similar to the rest of the world—desert dust and shamaal-wind particulate matter. Noted indoor-exposure killers are AC-dried, cool air, new incense and bakhoor smoke, and mold due to inadequately maintained cooling systems. Known food exacerbants are those that trigger reflux and those that dry the pharynx: fatty, fried, or leftover and ‘heavy’ evening meals, chocolate, mint, caffeine, and carbonated beverages.
Keep track of symptoms faced against exposures for two weeks to identify your personal triggers.
Can chronic cough be prevented?
View Answer
Not necessarily, but most people who are committed to avoiding these three habits will not develop a chronic cough: avoid smoking and secondhand smoke, start treating reflux and allergy early versus waiting for months before treatment, be current on influenza and pneumonia vaccines. For those with existing asthma or allergies, these individuals’ controller medications can prevent the airway inflammation that makes a chronic cough.
Is prednisone good for a lingering cough?
View Answer
Oral prednisone is not recommended as empiric therapy for most causes of chronic cough and has potential side-effect issues with repeated use. One exception is eosinophilic bronchitis, where a brief course of inhaled – or sometimes oral – corticosteroids results in rapid improvement. For common UACS, asthma, or GERD cough, your physician should aim to give you first-line targeted medication rather than systemic steroids. Always listen to your physicians judgement with regard to your diagnosis.
Tried the standard path and your cough is still there?
A Tong Ren Tang TCM practitioner in the United Arab Emirates can investigate your cough pattern, review your current investigations, and determine whether a pattern herbal treatment approach is appropriate for you. Contact us for face-to-face and virtual consultations.
Medical disclaimer. This information is provided only as a general educational overview based on peer-reviewed clinical literature, and not as a medical diagnosis or treatment plan. Many different conditions can cause chronic cough, and a self diagnosis cannot be relied upon. Only a physician can give you a proper workup; you need a qualified TCM herbal practitioner to suggest a condition-specific herbal therapy based on your pattern diagnosis. The red-flag symptoms noted above require urgent doctor’s attention in person. Tong Ren Tang Gulf only provides clinical consultations but cannot prescribe remotely without an in-person intake.
References & Sources
- Chronic cough — Diagnosis and treatment — Mayo Clinic (2024)
- Chronic Cough: Causes & Treatment — Cleveland Clinic (2024)
- Chronic cough: A review and prospects — PMC (2024)
- Chronic Cough in Adults: Make the Diagnosis and Make a Difference — PMC
- Management of chronic refractory cough in adults – PMC
- Chronic cough due to gastroesophageal reflux — CHEST 2016 guideline
- Clinical practice guide of Chinese medicine for cough (GRADE, 2023) – PMC
- Acupuncture-related therapy for chronic cough — systematic review — PMC
- Indoor Air Pollutants and Health in the United Arab Emirates – PMC
- Treating and Managing Chronic Cough – American Lung Association
- Solving Your Chronic Cough — Symptoms, Diagnosis & Treatments — University of Utah Health (2025)
About the reviewers.
This article was assembled by the Tong Ren Tang Gulf editorial team and clinically validated by members of the Tong Ren Tang TCM clinical team, utilizing 355 years of Tong Ren Tang pharmacy knowledge (established 1669, past Royal Court pharmacy to eight Qing dynasty emperors) brought together with up-to-date peer-reviewed respiratory papers. This content mirrors the CHEST 2016 expert panel position, Mayo Clinic and Cleveland Clinic treatment formats, and the WHO Traditional Medicine Strategy 2025-2034.