Get in Touch with Tongren Tang Gulf

Quick Specs
| Best-supported timing | 25 minutes before + 25 minutes after embryo transfer (Paulus 2002 protocol) |
| Effect on clinical pregnancy rate | RR 1.31 (95% CI 1.13–1.52) vs sham — pooled across 65,388 women |
| Effect on live birth rate | RR 1.10 (95% CI 0.86–1.41) — not statistically significant in 2025 meta of 22 RCTs |
| Strongest beneficiary subgroup | Women under 35 (RR 1.41) |
| Subgroups where evidence does NOT support adjunct use | Infertility duration ≥ 4 years (RR 0.81), embryos transferred ≥ 2 (RR 0.79) |
| Recommended protocol length | 8–12 weeks pre-cycle, ≥ 20 sessions for the strongest signal in 2025 evidence |
| Forbidden points in pregnancy | LI4, SP6, BL60, BL67, GB21 (per classical TCM and modern reviews) |
| Typical Dubai pricing range | AED 200–450 per session; AED 150+/session in 5–10-session packages |
What Twenty Years of Trials Tell Us About Acupuncture and IVF

A guidewire honest dialogue regarding acupuncture and IVF success begins with a 2002 study. Wolfgang Paulus et al., publishing in Fertility and Sterility, randomized 160 women to assisted reproduction therapy. Eighty received a pre- and post-embryo transfer acupuncture treatment 25 minutes apart; the other eighty received standard treatment. Clinical pregnancies were reported in 34 of 80 women (42.5%) undergoing acupuncture, and 21 of 80 women (26.3%) receiving standard care. That two-session protocol has since served as the template for twenty years of follow-up trials.
Things become murkier after Paulus. Manheimer et al’s 2008 meta-analysis pooled 13 trial of 2,500 women, and found a statistically non-significant relative risk of 1.34 for live birth (95% CI 0.85-2.11). A 2013 Cochrane review by Cheong et al concluded: “There is no evidence that acupuncture improves live birth or pregnancy rates in assisted conception.” Then 2018 JAMA paper by Smith et al-the largest single trial ever-wound the clock back: 824 women, live birth 18.3% in the acupuncture, versus 17.8% in the sham control group, non-the statistically non-significant 0.5% difference.
The largest and most-current synthesis by Wang et al, Frontiers in Public health, published in 2021, used 16 systematic reviews, 312 underlying randomized trials, and 65,388 participants. Compared with sham, real acupuncture increased significantly clinical pregnancy rate (RR 1.31, 95% CI 1.13-1.52, p=0.0004). Live birth, ongoing pregnancy, biochemical pregnancy, and miscarriage had no significant differences when compared to sham-acupuncture. In 2025, Yang et al, pooling 22 RCTs in 3,677 patients from across 7 countries found a similar pattern clinical pregnancy improved (RR 1.26, 95% CI 1.08-1.47), live birth did not (RR 1.10, 95% CI 0.86-1.41).
“Women asking if acupuncture will improve their IVF want a yes or no. A truthful response is yes in regard to clinical pregnancy and uncertain in regard to live birth-and that difference alone presents such a positive clinical message that it should be addressed in any conversation about acupuncture with a fertility specialist. ”
Significance. Twenty years of trials produce a directional but qualified conclusion: acupuncture can improve clinical pregnancy rates, the impact on live birth remains equivocal, and though one upswing patient literature sounds encouraging, single trials alone do not warrant confident enthusiasm.
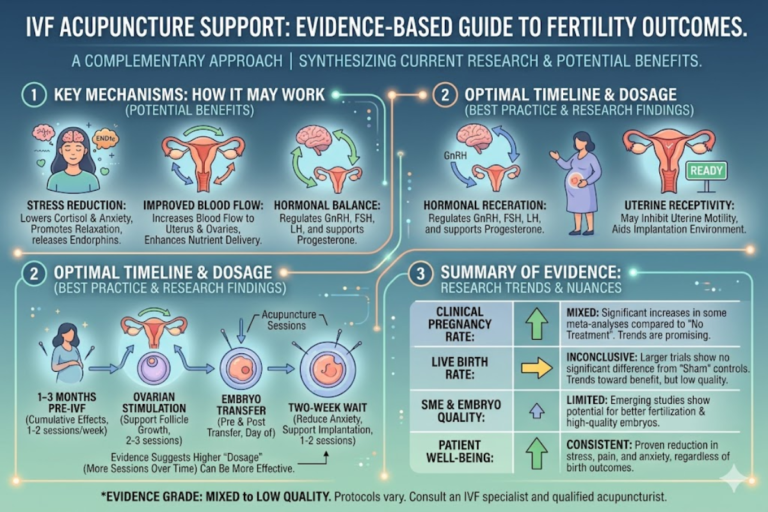
Four Mechanisms by Which Acupuncture May Influence IVF Outcomes
So if acupuncture does influence clinical pregnancy rates, what is a likely physiological pathway?
There are at least four mechanisms that feature prominently in the literature of reproductive medicine:
1. Increased blood flow to the uterus and ovaries
The 1996 paper by Stener-Victorin et al. still provides the clearest mechanism of action in Human Reproduction. Eight sessions of electro-acupuncture were administered to ten infertile women with increased impedance to flow in the uterine arteries and significantly reduces the mean pulsatility index of the uterine arteries were observed from a pre-treatment value of 2.3-2.4 to a post-treatment value of 2.0-2.2 and continue to show significant reduction 10-14 days later. a reduction in pulsatility index indicates a reduction in resistance and consequently more nutrients in blood to the endometrium in the window of implantation.
2. Modulation of the hypothalamic-pituitary-ovarian axis
Acupuncture seems to modulate reproductive hormones through the hypothalamic-pituitary-ovarian axis (HPO) during stimulation. The autonomic pathways of the sympathetic nervous system seem most to be involved. A reduction in the central sympathetic outflow can result in dilation of uterine and ovarian vessels, and may also dampen the cortisol response during stimulation cycles.
3. Endogenous opioid release and stress reduction
Needling stimulates the release of β-endorphin and other endogenous opioids, producing the subjective “acu-stoned” sensation many patients report. For women undergoing IVF — a process associated with high stress and anxiety — that subjective relaxation effect is reproducible and well-documented. In 2025, University Hospitals reported that acupuncture significantly relieved stress and pain in women undergoing IVF, regardless of pregnancy outcome.
How Does Acupuncture Work Scientifically?
Contemporary reproductive medicine no longer employs the metaphysics of manipulating qi flow, but measures the peripheral neural response evoked by acupuncture (cutaneous afferent nerve stimulation) and subsequent downstream biological effects: alteration in autonomic balance involving stress hormones, as well as pelvic vasodilitation. In their 2021 review Wang et al put this into clinical perspective: stimulation of the skin-at even nonspecific sham points-activates cutaneous afferent nerves, producing a ‘limbic touch response’, and hence the difficulty in differentiating real from sham acupuncture in rigorous clinical trials.
4. Improvement in endometrial receptivity
Endometrial receptivity- cellular and immunological environment supportive for a successful implantation- relies on appropriate vascularization and cytokine signaling, and a correct progesterone response. All the three reasons above are directly involved in determining endometrial receptivity and this is the reason why a majority of protocol place acupuncture around the time of implantation rather than on egg-retrieval.
The take away. The four mechanisms seem to work at various levels – vascular, hormonal, neurochemical and receptivity at the tissue level but are focused on the same window of time: the day or so surrounding embryo transfer.
Optimal Timing: When to Schedule Acupuncture in Your IVF Cycle

“When do I begin acupuncture?” is second only to “Does it work?” The 2025 meta-analysis published by Yang and colleagues found the embryo culture period to be the most effective treatment period, with ovarian stimulation and ART preparation periods also producing equally useful results. More prolonged treatment periods (noted by the maximum of 3 months spent at 20 or more treatments) was preferable.
| Cycle phase | Timing | Frequency | Evidence anchor |
|---|---|---|---|
| Pre-cycle preparation | 8–12 weeks before stimulation | 1× weekly | Yang 2025 (≥ 20 sessions superior) |
| Ovarian stimulation | Days 1–10 of stimulation | 2× weekly | Westergaard 2006 / Yang 2025 |
| Egg retrieval | Day before retrieval | 1 session | Yang 2025 — modest effect at this phase |
| Embryo transfer (Paulus protocol) | 25 min before + 25 min after transfer | 2 sessions on the day | Paulus 2002 — the founding protocol |
| Luteal phase | Days 1–10 post-transfer | 1–2× weekly | Wang 2021 — sham-controlled CPR benefit |
How Many Acupuncture Sessions Do You Need for IVF?
A sincere reply, it boils down as to which research base you stand by. Paulus’s initial 2002 protocol consisted of a mere two sessions at transfer day. Hullender Rubin et al. 2013 retrospective chart review found no significant live-birth difference in non-donor cycles with that two-sessions approach alone (OR 1.04, 95% CI 0.68-1.57), but uncovered a 31% increase in live-birth among donor cycles (RR 1.31).
Conversely, Yang’s 2025 meta-analysis revealed that perhaps 20 or more sessions over a minimum of three months – that being weekly sessions for 8-12 weeks pre-cycle and transfer day acupuncture – yielded the most compelling evidence. For the forward-looking patient utilizing this as an effective adjunct, that equates to 16-25 sessions in an entire IVF cycle, costing around AED 3,000- AED 11,000 in Dubai depending upon package options.
Main point. Two transfer day treatments are not nothing, but they are not the dose where the published benefit is largest. To your acupuncturist who recommends only then-day-of transfer protocol, ask: why? 2025 evidence indicates a longer pre-cycle window.
The Acupuncture Points Used (and Those Avoided in Pregnancy)
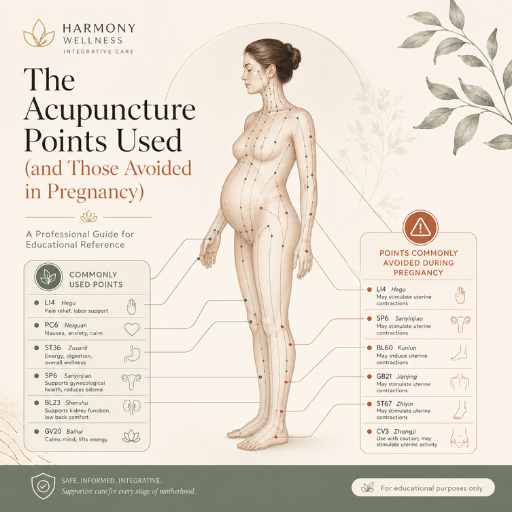
Most current published IVF acupuncture protocols are based on one or two traditional sources. The modern Western reference point for the two Paulus 2002 and Stener-Victorin protocols is based on previous use of our own modern classical TCM gynecological counterindication list. Whatever the design, the points have a common framework of three functional blocks: blood-and-qi-supplementing points on the legs and lower abdomen, calming and anxiety-reducing points on the head and ears, and spleen-and-liver-channelpoints to maintain the underlying architecture of the menstrual cycle.
Commonly cited body points in IVF acupuncture include SP6 (Sanyinjiao) on the inner ankle, SP8 on the inner calf, ST29 (Guilai) on the lower abdomen, CV4 and CV3 on the midline below the umbilicus, and PC6 (Neiguan) on the inner forearm. Auricular points such as Shenmen and Zigong are often added on transfer day for relaxation and uterine focus.
What Are the 5 Forbidden Acupuncture Points in Pregnancy?
The five points traditionally avoided during pregnancy due to “intense qi-moving or descending” effect are LI4 (Hegu on the hand between the thumb and forefinger);SP6 (Sanyinjiao on the medial side of the lower leg just on the inside of the ankle);BL60 (Kunlun on the posterior side of the lateral aspect of the ankle);BL67 (Zhiyin on the lateral side of the smalltoe); and GB21 (Jianjing on top of the shoulder). Meta-analyses of modern controlled trials considered by Carr in 2015 (a study that has been cited 49 times) have come to the conclusion that, when used to treat non-obstetric pain conditions, needling at these “forbidden” points does not have an effect on adverse pregnancy outcomes, though clinicians still tend to avoid them in practice once pregnancy is confirmed. A pragmatic practice argument: a dedicated fertility acupuncturist, adequately trained, would tend to administer needling at SP6 for the IVF cycle planning and cease once pregnancy is confirmed by negative or positive beta-hCG.
📐 Engineering Note
Needle gauge in IVF acupuncture protocols tend to be 0.18-0.25 mm diam, about 40 time thinner than a hypodermic. All licensed clinics use disposable single-use stainless steel needle that meet the safety standards set by ISO 17218:2014. The depth of the needle inserted at SP6 tends to be about 10-25 mm. at ST29 20-40 mm.
Key takeaway. Point lists matter less than practitioner training. A clinician who cannot explain to you why SP6 is on their fertility list and not on their pregnancy-confirmed list is a clinician who cannot calibrate.
Who Benefits Most? Fertility Subgroups Where Evidence Is Strongest (and Where It Is Not)

This is where the 2021 Frontiers in Public Health broadsheet turns into the best article in the corpus. Wang and team subgrouped the 65,388-patient pooled data pool based on protocol and patient features with outcome measures directly contradicting the all-too-common “more is more” myth.
| Patient subgroup | Effect on clinical pregnancy | Recommendation strength |
|---|---|---|
| Age < 35 | RR 1.41 (1.15–1.74) | Supportive — clearest evidence base |
| Age ≥ 35 | RR 1.15 (0.85–1.54), NS | Inconclusive — proceed if affordable |
| Infertility duration < 4 years | RR 0.98 (0.84–1.13), NS | Inconclusive |
| Infertility duration ≥ 4 years | RR 0.81 (0.71–0.93) | ⚠ Not supported — pooled effect was detrimental |
| Embryos transferred < 2 | RR 1.02 (0.92–1.13), NS | Inconclusive |
| Embryos transferred ≥ 2 | RR 0.79 (0.70–0.88) | ⚠ Not supported — pooled effect was detrimental |
| Unexplained infertility | Modest positive in some Manheimer subgroups | Reasonable adjunct trial |
| PCOS | Mixed: Karolinska 2018 negative for primary fertility, Frontiers 2024 positive in subset analyses | Highly individual — discuss with both your RE and an experienced TCM practitioner |
Both detrimental subgroups deserve more thought than they usually receive. Long infertility duration (≥ 4 years) typically signals more profound underlying pathology — diminished ovarian reserve, severe endometriosis, deep tubal disease — where any peripheral neural stimulus is unlikely to overcome the mechanical or biological barrier. Multiple-embryo transfers carry independent biological complexity around uterine contractility and competing implantation, which acupuncture’s relaxant effect may not help.
For male-factor cases, the picture is more cautiously optimistic. Acupuncture has been associated with improvements in sperm motility and concentration in several small randomized trials. In a 2005 study of 28 men with idiopathic infertility, post-acupuncture quick sperm motility improved from 11.0% ± 7.5% to 18.3% ± 9.6% (p < 0.01). Translation into actual ICSI or IVF live birth gains, however, has not been consistently demonstrated at meta-analysis scale.
Decision architecture. If you are less than 35 years old, if the presumption of conception is less than four years then evidenced designed for a single-embryo transfer attempt would corroborate with a measured addition of acupuncture as a structural adjunct adjunct. If you are greater than 35 and have been conceiving for greater than four years, do not fall prey to the fads of atherotenicprogram replacing or delaying your reproductive endocrinologist’s prescription. Use the acupuncture for symptom relief and stress relief, not as an efficacy signal.
You can read more about fertility acupuncture in Dubai, our approach to PCOS-related fertility challenges, the cycle-regulating role of menstrual irregularity treatment, and complementary male partner fertility support — particularly relevant for couples preparing for ICSI cycles.
Why the Trials Disagree: The Sham Acupuncture Problem

If acupuncture works, why did the largest single RCT — Smith and colleagues 2018 in JAMA — find no effect? And why does the National Center for Complementary and Integrative Health summarize the 2021 review base by saying “no difference was found between the acupuncture and sham acupuncture groups in rates of pregnancy or live birth”? An answer lies in a methodological pothole most fertility blogs skip past entirely: sham acupuncture is itself a physiologically active treatment.
Wang’s 2021 overview of systematic reviews stated the issue plainly. Needling sham points still “evokes activity in cutaneous afferent nerves and leading to the ‘limbic touch response,’ so they were equally effective.” When the placebo arm receives an active intervention disguised as inert, any real-vs-sham trial systematically underestimates the true effect size of the verum treatment. Splitting their pooled estimates by sham type, the same authors found that invasive sham controls produced an apparent acupuncture benefit of RR 1.77 (95% CI 1.09–2.86), while non-invasive sham produced a smaller RR 1.28. Whichever kind of placebo you choose changes the answer you get.
“The view that acupuncture increased chances of becoming pregnant was probably wrong.”
An honest reading is not that one camp is right and the other wrong. Both findings are real: 2018 JAMA showed no difference; 2021 Frontiers’ pooled result showed RR 1.31 against sham. Both findings can co-exist if you accept three things: (1) the average effect of acupuncture on live birth is small enough to be hidden by trial heterogeneity; (2) sham controls are not inert; (3) protocol dose and patient subgroup matter more than headline averages, which is precisely what the subgroup data in the previous section showed.
Key takeaway. “Acupuncture doesn’t work in IVF” and “acupuncture works in IVF” are both rhetorical positions. A research-faithful position is: effect size is modest at best, depends heavily on dose and subgroup, and is partially obscured by a sham-control problem that fertility journalism rarely explains.
TCM Beyond Needles: Herbs, Diet, and Lifestyle in Fertility Support

Acupuncture is one tool in a broader Traditional Chinese Medicine system that also includes herbal formulas, dietary therapy, and lifestyle counseling. Whole-Systems TCM trials — which combine these tools rather than isolating acupuncture — tend to show larger and more consistent fertility benefits than acupuncture-only trials, though the evidence base is smaller and harder to interpret. In 2025, University Hospitals concluded that Whole-Systems TCM provided meaningful symptom relief during IVF.
Classical Chinese herbal formulas relevant to fertility include Bushen Huoxue Tang (kidney-tonifying, blood-moving) and Wenjing Tang (warming the menstrual cycle architecture). These are dispensed by trained practitioners who individualize the formula by tongue, pulse, and cycle pattern — not as off-the-shelf supplements. Chinese herbal formulas for fertility require careful coordination with your IVF medication schedule because of interactions between certain warming herbs and gonadotropin protocols. For a broader introduction to the principles, see our Chinese herbal medicine principles overview.
Important safety note. Do not start any herbal formula in the four weeks before stimulation without informing your reproductive endocrinologist. Some herbs influence estrogen-receptor activity; others affect platelet aggregation. Coordination is the difference between adjunctive support and pharmacologic interference.
Choosing a Practitioner and What to Expect: Cost, Sessions, Credentials

Published trials use practitioners trained at standardized levels — typically a four-to-five-year university degree in Traditional Chinese Medicine, licensure by a state or national board, and post-graduate training in reproductive medicine. In Dubai, fertility acupuncture practitioners are licensed by the Dubai Health Authority (DHA), which audits the underlying TCM degree and clinical hours. An American Board of Oriental Medicine fellowship is another credential signal in the U.S. and global market — fellows pass a board examination and maintain continuing education in reproductive cases.
Is Acupuncture for Fertility Worth It?
Absolute evidence should be matched to expectations. Benefits (in clinical pregnancy rate) from published trials average in the order of 25-30% in relative terms-66% !. This is tangible but by no means definitive.
It translates to a few percentage points absolute benefit in a 30% per cycle auto-discontinuedlive birth probability, for example. Whether such benefit warrants reaching an AED 3000-AED 11,000/session level depends on many factors and, evidently, on individual value judgements, including your available budget, whether you can allow your self time in the midst of an already heavy cycle, and whether you feel the well established stress alleviation, regardless of pregnancy outcome, is worth it for you. For some women, the answer is unobjectionably positive.
For others- especially those in the subset in which all pooled data pointed to no benefit- the value/evidence ratio is less defensible.
How Long Does It Take for Acupuncture to Help Fertility?
Yang’s 2025 meta-analysis found the strongest signal at protocols lasting at least three months and at least 20 sessions. Allow for an 8- to 12-week pre-cycle timeframe leading up to the start of ovarian stimulation by the reproductive endocrinologist. Subjective benefits evidenced by improvements in sleep, cycle pain, anxiety are usually registered within 2-4 sessions.
Returfoof changes in uterine artery flow noted after 8 sessions in the Stener-Victorin studies. Differences in pregnancy outcomes do not seem to appear until the completion of the entire protocol.
💡 Pro Tip — Vetting an IVF Acupuncturist
Ask 3 questions prior to booking.
1. Have you trained specifically in reproductive TCM and what does that look like? a fellowship, a board exam, post-graduate certification? 2. Will you communicate with my reproductive endocrinologist?
If so, that is a quality marker 3. “What is your protocol for women in their first IVF cycle?” An intelligent answer that cites either Paulus or Stener-Victorin protocols (not mere relaxation babble) will indicate serious reproductive-medicine training.
If you are evaluating clinics, our IVF acupuncture support program at our Dubai clinic offers DHA-licensed practitioners, coordination with your reproductive endocrinologist, and protocols based on the published evidence reviewed in this article.
Three Lower-Friction Ways to Get Started
- Download the Pre-IVF Acupuncture Protocol Guide — a printable session-by-session calendar matched to a typical Dubai IVF schedule.
- Take the brief “Are You a Candidate for IVF Acupuncture?” self-assessment based on the subgroup evidence in this article.
- Send a WhatsApp question to a TCM practitioner — Jumeirah branch +971 50 828 3687, Dubai Healthcare City +971 50 246 4888.
Book an IVF Acupuncture Consultation →
2025–2026 Outlook: What Is Changing in Acupuncture-IVF Research
Three research directions are shaping the next generation of acupuncture-IVF evidence. First, the field is becoming multinational. Yang’s 2025 meta-analysis pooled trials from seven countries, breaking the historical pattern of China-dominated research and adding methodological diversity. Second, attention is shifting from the Paulus two-session transfer-day protocol toward longer dose protocols with embryo-culture-period emphasis. Third, “Whole-Systems TCM” — acupuncture combined with herbs, diet, and lifestyle — is being studied as a distinct intervention rather than a confounder.
For patients planning a 2026 cycle, three implications follow. If your acupuncturist’s protocol is still strictly day-of-transfer Paulus, ask whether they have updated to a 8-to-12-week pre-cycle approach. If you are considering Chinese herbal medicine, expect your reproductive endocrinologist’s coordination posture to be more permissive than five years ago, but still protocol-bound. And if you are reading a 2026 fertility blog whose only citations are Paulus 2002 and Smith 2018 — that is an outdated evidence stack. Wang’s 2021 Frontiers overview and Yang’s 2025 meta-analysis are the current Tier-1 anchors.
Frequently Asked Questions
Q: Does acupuncture the day of embryo transfer affect the clinical pregnancy rate?
View Answer
Paulus’s original 2002 protocol — 25 minutes before plus 25 minutes after embryo transfer — produced a clinical pregnancy rate of 42.5% versus 26.3% in the control group. Subsequent trials gave mixed results, with the largest 2018 JAMA RCT finding no live birth difference. Wang’s 2021 overview pooling 65,388 women found a sham-controlled clinical pregnancy benefit of RR 1.31, but no significant live birth difference. Day-of-transfer acupuncture is a meaningful, if modest, addition; longer pre-cycle protocols likely add more.
Q: Can acupuncture treatment affect sperm density in males with very low sperm count?
View Answer
Several small randomized trials have shown acupuncture improving sperm motility and concentration in men with idiopathic infertility — quick motility rising from approximately 11% to 18% in one 2005 trial. Whether those laboratory improvements translate into measurable IVF or ICSI live birth gains has not been consistently demonstrated. For couples planning ICSI, acupuncture as a male-factor adjunct is reasonable to consider but should not replace standard semen-quality optimization (lifestyle, weight, abstinence interval).
Q: When should you get acupuncture for fertility?
View Answer
Current 2025 evidence supports starting acupuncture roughly three months before ovarian stimulation, at one or two sessions per week, then continuing into the stimulation, retrieval, transfer, and luteal phases. Twenty or more sessions across the cycle was associated with the largest benefit signal. If your IVF cycle is already underway, day-of-transfer acupuncture using the Paulus protocol is still worth considering as a lower-investment option.
Q: Can acupuncture and IVF success rates change over time across different countries and protocols?
View Answer
Yes, and this is one reason synthesizing the literature is hard. Yang’s 2025 meta-analysis pooled 22 RCTs across seven countries and found heterogeneity across regions and protocols. National differences in IVF baseline success rates, acupuncture practitioner training standards, and patient demographics all shift the apparent effect. Cleanest interpretation: a relative improvement of around 25–30% in clinical pregnancy is the directional signal supported across multiple jurisdictions, with live birth effects more variable.
Q: If there is no real evidence acupuncture helps IVF success rates, is it harmful?
View Answer
For most women, acupuncture during IVF is not harmful when administered by a properly trained practitioner using sterile single-use needles. Carr’s 2015 review of forbidden-points safety found no increased risk of adverse pregnancy outcomes even at points classically avoided. Two cautions apply. First, the 2021 Frontiers subgroup data flagged worse pooled outcomes in women with infertility duration over four years and in cycles with two or more embryos transferred — discuss your specific case with your reproductive endocrinologist. Second, do not let acupuncture sessions replace evidence-based medical treatment — the harm is opportunity cost, not direct injury.
Q: Does acupuncture and traditional Chinese medicine really make a difference for fertility?
View Answer
A modest, qualified yes for clinical pregnancy. Wang’s 2021 overview of 65,388 women found acupuncture significantly increased clinical pregnancy rate versus sham (RR 1.31). Yang’s 2025 meta found a similar pattern (RR 1.26). Live birth evidence is mixed across analyses. Whole-Systems TCM — combining acupuncture with herbal medicine, diet, and lifestyle — has shown larger and more consistent benefits in smaller trials, but the evidence base is less mature. Set expectations to a measurable but moderate adjunct effect, not a replacement for medical IVF.
Methodology and Sources Behind This Review
This review was assembled by reading and cross-checking peer-reviewed randomized trials, systematic reviews, and meta-analyses on acupuncture and IVF published between 2002 and 2025. We prioritized Tier 1 sources — government, academic, and peer-reviewed journal — over commercial fertility blogs and practitioner websites. Where multiple meta-analyses disagreed, we cite the largest and most recent (Wang 2021, Yang 2025) as primary anchors and earlier work (Paulus 2002, Manheimer 2008, Cheong 2013, Smith 2018) as historical context.
Specific numerical claims in this article were verified against original abstracts via PubMed. Where a figure circulating in commercial fertility journalism could not be sourced to its claimed primary publication — for example, a “+65% odds” figure attributed to Manheimer 2008 — we present the actually verifiable effect estimate (Manheimer’s RR 1.34, 95% CI 0.85–2.11) rather than the inflated claim. Pricing data reflects Dubai-market context as of Q2 2026 and may not reflect current rates.
Conflict of interest disclosure. Tong Ren Tang Dubai offers acupuncture and TCM services. This review was compiled from independent peer-reviewed literature; clinical claims throughout are linked to their source studies. Last reviewed April 2026; next planned update Q4 2026.
References & Sources
- Paulus WE, Zhang M, Strehler E, El-Danasouri I, Sterzik K. Influence of acupuncture on the pregnancy rate in patients who undergo assisted reproduction therapy. Fertil Steril. 2002;77(4):721-4 — Fertility and Sterility (Elsevier).
- Smith CA, et al. Effect of Acupuncture vs Sham Acupuncture on Live Births Among Women Undergoing IVF. JAMA. 2018;319(19):1990-1998 — JAMA Network.
- Manheimer E, et al. A systematic review and meta-analysis of acupuncture in IVF. 2008 — PubMed.
- Cheong YC, et al. Acupuncture and assisted reproductive technology. Cochrane Database Syst Rev. 2013 — Cochrane Library.
- Wang X, et al. An Overview of Systematic Reviews of Acupuncture for Infertile Women Undergoing IVF and Embryo Transfer. Front Public Health. 2021;9:651811 — Frontiers in Public Health.
- Yang Y, et al. Acupuncture for women undergoing IVF: an updated meta-analysis. 2025 — PubMed (Elsevier journal).
- Stener-Victorin E, et al. Reduction of blood flow impedance in the uterine arteries of infertile women with electro-acupuncture. Hum Reprod. 1996;11(6):1314-7 — Oxford University Press.
- NCCIH. Acupuncture: Effectiveness and Safety — U.S. National Center for Complementary and Integrative Health.
- Carr DJ. The safety of obstetric acupuncture: forbidden points revisited. Acupunct Med. 2015 — PubMed Central.
- Hullender Rubin LE, et al. Acupuncture and IVF: A Retrospective Chart Review. 2013 — PubMed Central.
- WHO. Acupuncture: Review and Analysis of Reports on Controlled Clinical Trials. 2003 — World Health Organization.
About This Evidence Review
This 2026 review of acupuncture and IVF success rates was compiled at Tong Ren Tang Dubai’s clinical content team — a DHA-licensed acupuncture and TCM practice operating from Jumeirah Road and Dubai Healthcare City. Conclusions reflect peer-reviewed evidence to April 2026, not in-clinic outcome data. For protocol-level questions specific to your IVF cycle, speak directly with a DHA-licensed practitioner who can review your reproductive endocrinologist’s plan.
Related Articles
- IVF Acupuncture Support Program at Tong Ren Tang Dubai — DHA-licensed protocol overview and booking.
- Fertility Acupuncture in Dubai — Treatment Page — for patients exploring fertility support before deciding on IVF.
- PCOS Treatment in Dubai with TCM and Acupuncture — for patients with the PCOS subgroup considerations discussed above.
- Menstrual Cycle Regulation and Pain Treatment — cycle architecture is the foundation of fertility readiness.
- Chinese Herbal Medicine: A Complete Guide to Principles, Herbs, and Evidence — background on the broader TCM toolkit referenced in this article.
- Perimenopausal Health and Fertility Considerations — for women approaching the upper range of IVF candidacy.