Get in Touch with Tongren Tang Gulf
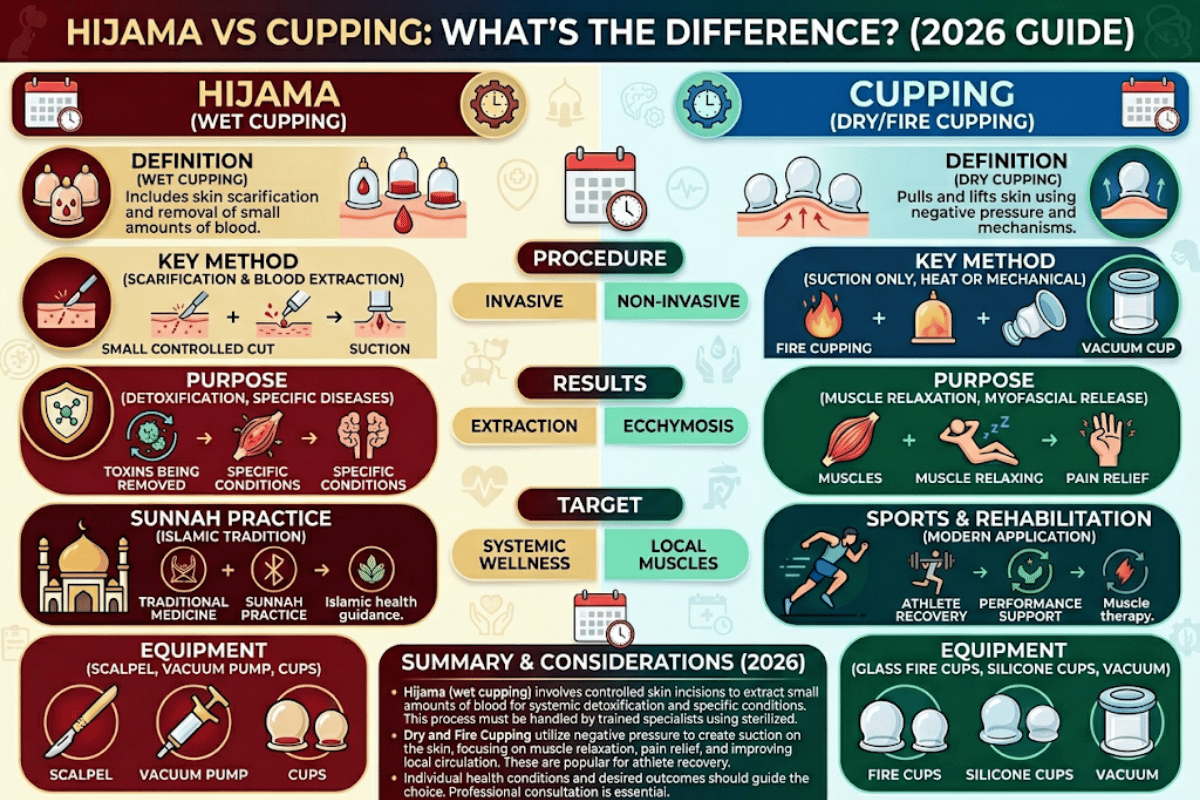
Short answer to hijama vs cupping: hijama is one type of cupping that sucks blood through tiny cuts in the skin, whereas common “dry” cupping just uses suction without any penetration. Both look exactly the same on a Michael Phelps action shot, but procedures, historical traditions, evidence base, and safety profiles differ in seven specific ways—and selecting the wrong method to achieve your goal can be a waste of time, and in the case of unregulated wet cupping, potentially dangerous.
This guide lays out the two practices side-by-side, citing peer-reviewed evidence on the efficacy of cupping (Cramer 2020, the 2024 low back pain meta-analysis, Cleveland Clinic) — including the benefits of cupping for pain and inflammation — the historical concepts behind each practice (the word hijama in Arabic translates roughly to “drawing out”), and the cupping therapist-specific details that can influence whether the outcome is therapeutic or harmful. Reviewed and critiqued by the TCM heritage team at Tong Ren Tang— a lineage that has performed cupping continuously since 1669.
Quick Specs: Hijama vs Cupping at a Glance
| Hijama (wet cupping) | Suction + 1–3 mm sterile lancet scratches; 30–100 ml blood drawn |
| Dry / fire cupping | Suction only; no skin break, no blood |
| Typical session | Wet 30–45 min; dry 10–20 min |
| Typical UK fee | £45–62 per wet session; dry sometimes lower |
| Recovery | Bruising 7–14 days (wet); 3–7 days (dry) |
| Strongest evidence for | Chronic pain, low back pain (2024 meta-analysis, high-to-moderate quality) |
What Are Hijama and Cupping? Plain-Language Definitions
Cupping is a family of therapies in which a specialist applies small cups to the skin and uses fire or a small pump to create a vacuum within each vessel. This vacuum pulls skin and a small amount of blood into the cup, creating the recognizable circular prod marks. The practice originated in both China and West Asia centuries ago, and the Chinese word ba guan ( ) literally means “pulling a jar.”
Hijama is exactly 1 species of cupping: the wet species in which the practitioner uses a sterile blade to carve 1-3 mm points in the skin, then reapplies the suction so the vacuum sucks a limited quantity of blood into the cup. Etymologically, hijama derives from the root hajm, “to attract” or “to be absorbed.” Therefore, while every Hijama or hijama session is a cupping session, not all cupping sessions are hijama. At Tong Ren Tang, where TCM cupping has been practiced under one unbroken lineage since 1669— spanning eight emperor reigns and 188 years of feeding Qinge elite— the dry-cupping variations predate the biblically inspired wet practice, even though both modalities use the same physical tools.
This distinction matters because almost every algorithmic decision on practicalities— what kind of data is relevant, what are the risks involved, what a patient can expect afterwards, even how much it costs— hinges on whether blood is drawn. Here, the differences are illustrated in seven dimensions that can help you choose the optimal modality for your personal goal.
Hijama vs Cupping: 7 Core Differences at a Glance

Use the table as the 7-Difference Decision-making cycle to determine what sort of cupping suits you most. Every row is a common question meant to inform clinical investigation in one or more dimensions, and every box contains a concrete answer.
| # | Dimension | Hijama (wet cupping) | Dry / fire cupping (TCM) |
|---|---|---|---|
| 1 | What happens to skin | Suction + controlled superficial scratches (1–3 mm) made with a sterile lancet | Suction only — skin is pulled into the cup but never broken |
| 2 | Blood drawn | 30–100 ml typical per session, captured inside cup | None |
| 3 | Religious / cultural origin | Islamic Sunnah — recommended in Prophetic medicine; widely practiced across Muslim-majority regions | Chinese TCM canon (3,000+ years) and parallel traditions in Egypt, Greece, and other ancient cultures |
| 4 | Tools required | Cups + sterile single-use lancet/scalpel + biohazard sharps disposal + gloves | Cups + flame source or hand pump; reusable cups after sterilization |
| 5 | Typical session length | 30–45 min (includes the dry-cupping phase first) | 10–20 min for a focused area; longer if running cupping with oil |
| 6 | Recovery window | 7–14 days for round bruise marks plus scratch healing | 3–7 days — bruise only, no break in skin to heal |
| 7 | Regulatory status (West) | Higher scrutiny — UK practitioners flagged for regulation by the BBC in 2014; some US states require licensure for the bleeding step | Generally permitted under existing massage, acupuncture, or PT licenses |
Why the framework matters in practice: if you’re thinking about cupping as a sports recovery tool (the Phelps use case), dry cupping covers it. If you want the form recorded in Prophetic medicine and traditional Middle Eastern health care, that is hijama specifically — and the bleeding step is part of the practice, not an optional addition. Different types of cupping suit different goals.
Types of Cupping: Dry, Wet (Hijama), Fire, Facial & Moving

“Cupping” used in clinical practice describes a family of techniques. Five matter to most people:
Dry Cupping (Static Suction)
Applying glass cups or silicone suction cups on the back, shoulders, or affected area, then using a flame or a simple hand pump for creating a vacuum inside the cup. Cups remain in place for 5–15 minutes. Suction increases local blood flow and blood circulation underneath the cup, the proposed mechanism behind the pain relief and muscle-relaxation therapeutic effect. This is the most common form for muscle tension, sports recovery, and general relaxation, and it is the only form practiced by the Chinese Tong Ren Tang lineage that persisted through the Qing dynasty.
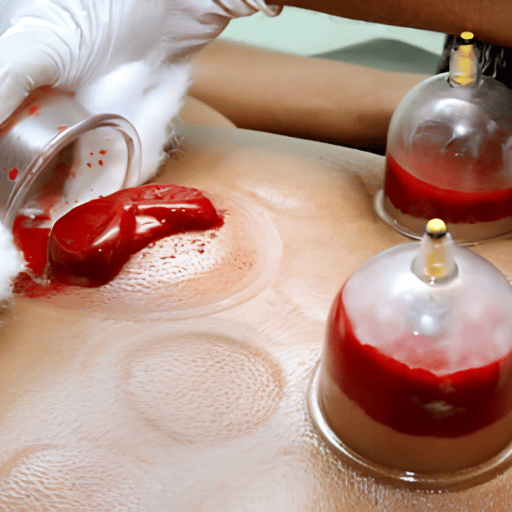
Wet Cupping / Hijama (Suction + Lancet)
A two-step cupping technique. First, dry cupping; then cups are removed, the practitioner scratches the skin at the desired location with a single-use sterile lancet, then cups are reapplied so the suction draws blood to the surface. Known as hijama in Prophetic medicine traditions, this is the modality supported by the most rigorous infection-control protocols — the broken skin provides a real bloodborne pathogen pathway and infection-prevention discipline matters to prevent infection.
Fire Cupping (Flame-Generated Vacuum)
Traditional Chinese medicine practitioners briefly ignite a cotton ball soaked in alcohol, swirl it inside the cup to deoxygenate the air, then place the cup on the skin so a vacuum forms as the air cools. Visually dramatic but functionally similar to mechanical-pump dry cupping. Carries an additional burn risk if the rim is heated and applied carelessly.
Facial Cupping (Lymphatic / Cosmetic)
Small silicone cups used on the face with short dwell times and very light pauses (less than 30 seconds on the same spot) so as to encourage lymphatic drainage without skin lift or bleeding. Not as focused as other forms of cupping, little suction and intended for cosmetic rather than medicinal purposes. Avoid areas with open or active acne.
Moving / Massage Cupping (Sliding with Oil)
Lotion or oil is applied to the skin, then cups are placed and slid along the muscle tissue with sustained suction — moving the cups combines the suction effect with myofascial release. Practitioners use this method as an alternative therapy for muscle tension and as a modern approach to combining traditional cupping with massage technique. Marks tend to be lighter and less circular because the cup never sits in one spot for long.
Where Each Tradition Comes From: Islamic Hijama vs Chinese Cupping

Cups themselves are older than either tradition’s claim to them. Egyptian medical texts, the Greek Hippocratic corpus, and pre-imperial Chinese silk manuscripts all reference some form of suction cupping. What separates hijama from broader cupping is the specific cultural weight that two distinct lineages place on the practice.
Hijama in Islamic tradition. Bleeding cupping is documented as part of Tibb an-Nabawi (Prophetic medicine) and is referenced in classical Hadith collections, including narrations attributed to Prophet Muhammad recommending the practice. Sahih al-Bukhari contains multiple hadith on hijama, and to this day many Muslim communities practice it on the 17th, 19th, or 21st of the lunar month based on tradition. From there, hijama spread along trade and pilgrimage routes through the Middle East, North Africa, and South and Southeast Asia, and is currently experiencing renewed clinical interest in academic research.
Cupping in Chinese tradition. Chinese ba guan has continuous documented use in TCM going back to silk medical manuscripts of the Han dynasty, and is integrated with acupuncture meridian theory. Cups are typically placed along the bladder meridian on the upper back, with point selection guided by the same pulse and tongue diagnostics that inform acupuncture and herbal prescriptions. Tong Ren Tang has practiced cupping under this lineage since 1669 — across the Qing imperial era, the Republican period, and into modern integrative medicine — making it one of the longest unbroken institutional records of cupping practice anywhere.
“Cupping therapy is a form of traditional medicine that originated in China and West Asia. People have practiced this method for thousands of years.”
— Cleveland Clinic, Health Library treatment overview
Cross-cultural footprint matters when choosing a practitioner. A TCM-trained acupuncturist defaults to dry cupping with meridian-based point selection. An Islamic hijama practitioner trained in the Sunnah tradition defaults to wet cupping at specific points described in classical texts (commonly the kahil at the upper back between the shoulder blades). Both are legitimate; they’re not interchangeable.
How Each Procedure Works: Step-by-Step Walkthrough
Understanding the actual mechanics removes most of the anxiety patients bring to a first session. Both procedures follow predictable sequences.
Dry Cupping Procedure
- Practitioner inspects the area, identifies treatment points (often along the bladder meridian on the upper back).
- Cups are warmed with flame and air (fire cupping) or air is drawn out with a hand pump (mechanical cupping).
- Cup is placed on skin; suction creates a localized vacuum, drawing skin and superficial tissue upward into the cup.
- Each cup remains in place 5–15 minutes (Cleveland Clinic notes 3–5 cups per session, up to 7 maximum).
- After the dwell time, cups are removed by breaking the seal at the rim. A round red mark remains and will fade in 3–7 days.
Wet Cupping (Hijama) Procedure
- Practitioner sterilizes the area with antiseptic and dons clean gloves.
- Dry cups are applied first, left in place 3–5 minutes to bring blood to the surface and mark the treatment area.
- After 3–5 minutes, cups are removed. Practitioner uses a single-use sterile lancet or scalpel to make 5–20 shallow scratches (typically 1–3 mm deep) in each treatment zone.
- Cups are immediately re-applied over the scratches, and the suction draws blood into the cup over the next 5–10 minutes.
- Cups are removed and inspected; the captured blood is typically 30–100 ml total across all cups, often with a clotted or sticky appearance.
- Sites are cleaned with antiseptic, dressed if necessary, and aftercare instructions are given.
- All sharps go directly into a regulated biohazard container — single use, no exception.
📐 Engineering NoteSuction pressure during cupping varies by device and practitioner — practitioner-reported ranges typically sit between -10 and -40 kPa (gauge pressure). Lancet penetration is intentionally superficial: depths greater than 3 mm increase bleeding without therapeutic gain and raise infection risk. Single-use sharps disposal follows WHO infection prevention and control standards for percutaneous procedures.
Does Hijama Hurt?
Most patients report dry cupping as a strong stretching or pulling sensation rather than pain — Cleveland Clinic notes the procedure “shouldn’t cause pain, though you may experience some skin tightness.” Wet cupping adds a brief, sharp scratch that practitioners commonly compare to a paper cut or a fingerprick blood test. Once the cups are reapplied, sensation returns to the same pulling feeling as the dry phase. Patients prone to fainting from needle sticks should mention this in advance — vasovagal syncope is the main acute risk, and a practitioner can position you reclined to reduce it.
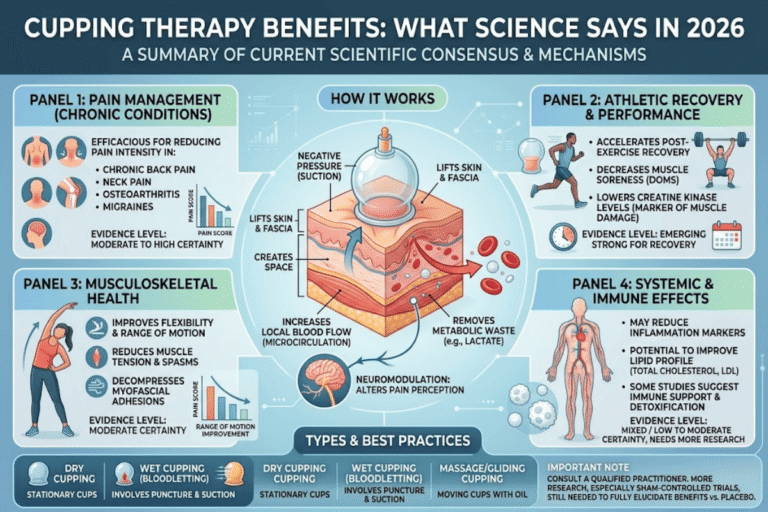
Conditions & Evidence: What the Research Says

Recent years have produced more high-quality studies into cupping than the previous three decades. What has emerged has been a mixture of effect size, but specific: cupping produces positive short-term effects for several pain conditions, and weak or non-existent evidence for many other claims made on commercial sites.
| Condition | Evidence grade | Recommended type |
|---|---|---|
| Chronic low back pain | B (high-to-moderate quality, 2024 meta-analysis) | Dry or wet — both supported |
| Chronic non-specific pain | B (Cramer 2020 J Pain meta-analysis, cited by 58) | Either; short-term effect documented |
| Knee osteoarthritis & arthritis-related pain | C (small RCTs; included in Cleveland Clinic indication list) | Dry; site-specific point selection |
| Chronic musculoskeletal pain | B (PMC12121573, 2025 review) | Dry; supports immediate pain reduction |
| Migraine / tension headache | C (small RCTs, mixed results) | Wet (hijama) historically; evidence still developing |
| Asthma symptoms (adjunct) | C (PMC11407324, 2024 — reduced medication use observed) | Wet cupping in study protocol |
| Hypertension | C (small studies, some positive) | Wet historically; not a stand-alone treatment |
| Sports recovery | D (popular use, weak controlled evidence) | Dry — the Phelps-style use case |
The strongest single short-term effect demonstrated by recent reviews is from the 2024 systematic review of cupping for low back pain: “high-to-moderate quality evidence indicates that cupping significantly improved pain and disability.” That is unusual language in a cupping context–most reviews are cautious, but the 2024 review identified the methodologically rigorous trials has improved sufficiently to offer stronger recommendations.
As with all conditions, two caveats are relevant. First, almost all positive evidence is for short-term effects (weeks, not months). Second, sham control trials are difficult, due to the bruising: the bruising makes it impossible to blind the client, an important methodological weakness, which researchers are actively trying to work around; see, for example, the 2025 dry cupping vs placebo trial in the Journal of Orthopaedic & Sports Physical Therapy.
The evidence does not support any additional claims that cupping will cure cancer, resolve infertility, remove ‘toxins’ as defined medically, or replace any evidence-based treatment for a serious condition. Some commercial sites make those claims, but peer-reviewed literature does not.
Safety Profile: Risks, Side Effects & Contraindications

wet cupping involves the taking of blood, but it’s not phlebotomy, and that distinction is probably of more importance to safety than the practitioner’s pain. Federal registered phlebotomists work under hospital infection control and using their professionally sterile environment, draw blood from veins into vacuum-sealed tubes. A hijama session creates 5-20 superficial skin breaks, and the risk of a session depends just as much on whether the practitioner performs your breaks with the same discipline as a phlebotom.
Risk for dry cupping is mild. The risk of wet cupping in unlicensed settings is real,and a 2014 review by Rehman et al in the American Journal of Infection Control documented that hijama is a definitive risk factor for hepatitis C transmission, with a pooled odds ratio of 1.5 across the studies reviewed and 24,948hepatitis C cases included in one of the analyses surveyed.
⚠️ Documented risks
- Blood borne pathogen transmission (HIV, HBV, HCV) – wet cupping only, when sharps are reused
- Bacterial skin infection at scratch sites – wet cupping only
- Bruising – universal, resolves in7-14 days for wet, 3-7 days for dry
- Vasovagal syncope (fainting) – most common during the bleeding step
- Burns from heated cups — fire cupping only
- Anemia — rare, with frequent high-volume wet cupping
⚠ Avoid cupping if you have
- Pregnancy (insufficient research)
- A pacemaker
- Bleeding disorders (hemophilia)
- Anticoagulant medication
- Active deep vein thrombosis or stroke history
- Cardiovascular disease
- Active eczema, psoriasis, or other skin condition at the site
- Severe anemia
- Seizure disorders (epilepsy)
Contraindications listed above are consolidated from Cleveland Clinic’s published guidance. If you take a daily blood thinner, have any of the conditions listed, or are unsure, talk to your physician before booking – that conversation takes five minutes and is the single most useful safety step you can take.
📐 Engineering NoteSterilization protocol that meaningfully reduces blood borne pathogen risk:single-use sterile lancets sourced from medical-grade suppliers,single-use cups for wet cupping (or autoclaved between patients with documented sterilization log),individually packaged gauze and antiseptic wipes,regulated sharps container at point of use,and gloves changed between patients. This is the same standard expected of acupuncture clinics,tattoo studios,and any setting where percutaneous procedures occur.
Aftercare: Recovery Timeline & Practical Do’s and Don’ts

Recovery after dry cupping is mostly about waiting for the bruise marks to fade. Recovery after wet cupping has the additional task of letting small skin breaks heal cleanly. A seven-day window covers both, mapped out below.
First 24 Hours
- ✔
Drink water steadily- recovery is easier when you’re well hydrated, particularly after wet cupping. - ✔
Keep the treated area covered and dry for the first 4-6 hours after wet cupping; loose clothing helps. - ✔
Eat a light,nourishing meal within an hour or two- many patients feel mildly tired after a session. - ✔
Rest. Cupping is not the day for an intense workout, alcohol, or a sauna.
Can I Shower After Wet Cupping?
Most practitioners advise waiting at least 6-24 hours before showering after wet cupping, and avoiding hot water, hot tubs, swimming pools, and saunas for 48 hours so the small scratches stay clean and dry while they close. After dry cupping there is no skin break, and a normal shower is fine the same day; just avoid scrubbing the bruised area with abrasive sponges or hot water.
Days 2–7
- ✔
Resume normal activity as your energy returns; light walking and stretching are fine from day 2. - ✔
Bruise marks will shift from dark red to brown to yellow-green and fade by day 7-14. - ✔
Watch the wet cupping sites for redness, warmth, swelling, or discharge- call your practitioner or doctor if any of these appear,since these are early signs of infection. - ✔
Iron-rich food (leafy greens, beans, red meat) supports recovery if you have had a higher volume wet session.
What to avoid: Do not put ice or heat directly on the bruise sites in the first 24 hours, do not pick at scabs, and do not schedule back-to-back wet cupping on the same body area within 14 days.
How to Choose a Qualified Practitioner

Practitioner selection is the single largest variable in cupping outcomes. An educated acupuncturist in a clean, regulated clinic using single-use lancets is a very different animal to an unregulated mobile ‘doctor’ who makes house calls with reusable equipment, and the safety disparity is appalling. Use the following audit before you book.
10-Point Practitioner Audit
- Formal health licensure or certification published in the clinic (acupuncture license, hijama certification, or relevant medical credential).
- For wet cupping: written sterilization protocol available on request.
- Sealed, single-use lancets opened in front of you.
- Sharps receptacle in view at the treatment table.
- Gloves changed between patients (and ideally between procedure stages).
- Autoclaved cups for wet cupping with an accessible log.
- Practitioner inquires about your medical and contraindication history.
- Clear written aftercare instructions provided post-session.
- Realistic scope of practice claims – no guarantees to cure cancer, autoimmune disease, or to replace prescribed medication.
- Transparent pricing, including any per-cup or extra-area fees.
Cost Benchmarks (2025)
Pricing in the table below varies considerably depending on market size (UK, US, and Singapore statistics cited below are based on practitioner figures from public sources, not market studies) and competition in an area. Use this as a benchmark for what most consumers should expect to be paying for a standard service at a controlled clinic.
| Market | Dry cupping | Wet cupping (hijama) |
|---|---|---|
| United Kingdom | £40–80 | £45–62 per 45-min session (commonly), up to £75+ for extended sessions or many cups |
| United States | $30–80 (practitioner-typical) | $80–200 (practitioner-typical, varies by state and licensure) |
| Singapore | S$50–150 (practitioner-typical) | S$80–250 (practitioner-typical) |
UK prices are based on published clinic price lists; US and Singapore prices are based on average practitioner rates from publicly available sources instead of market surveys. You can treat these figures as a benchmark for your local market, but do not expect them to be representative of what is actually out there.
BBC News warned in 2014 that skilled UK practitioners of hijama had been calling for regulation citing the systematic mismatch between the blood letting nature of the procedure and the consumer-facing notion that it should be in the same category as massage, was stark. That gap has been partially closed off in some parts of the world and is still all but unrecognizable in others. Check locally before booking a therapy service into any specific regulatory framework.
Industry Outlook: Modern Research, Olympic Adoption & TCM-Western Integration

Cupping discourse has been evolving from “ancient curiosity” to “active research field” in less than a decade. This evolution was catalyzed by three factors: U.S. Olympic swimmer Michael Phelps making his iconic discoloration public, the accumulation of high-quality modern research and clinical trials through the late 2010s and early 2020s, and expansion of integrative medicine programs at academic healthcare institutions — which now treat modern medical perspectives on hijama and cupping as legitimate alternative medicine and complementary medicine research priorities rather than a closed case.
Business statistics confirm the same trend on a commercial level. Market data projects cupping therapy kits to expand from around $443 million in 2025 to $853 million in 2032 — reflecting a CAGR of 9.80% per one industry tracker. That growth mirrors the clinical research pipeline, with 2024’s low back pain meta-analysis explicitly reporting “high-to-moderate quality” evidence in this literature for the first time.
Phelps’s Olympic moment also delivered its own backlash — Forbes published a strongly critical piece by Steven Salzberg in 2019, and Skeptical Inquirer ran a follow-up arguing the Olympic visibility outpaced the science. Both perspectives are worth reading. The maturing 2024–2025 evidence base is starting to reshape the conversation, with a clearer separation between “well-evidenced for chronic pain short-term” — including conditions like fibromyalgia syndrome — and “weakly evidenced for everything else.” Modern medicine increasingly treats cupping as a defined intervention rather than an undifferentiated category.
For Tong Ren Tang — a TCM lineage practicing cupping continuously since 1669 — this shift is something the institution has been preparing for over centuries: cupping is moving from cultural artefact to evidence-graded practice, with the same diagnostic discipline Tong Ren Tang has applied to herbal medicine for hundreds of years. A 350-year corporate motto — “no compromise on cost and labour despite complexity, no compromise on quality and standard despite scarcity” — applies to cupping practice in 2026 the same way it has applied to herbal medicine since the Qing dynasty.
If you are considering cupping practice in 2026: read up on the guidelines in the 2024 LBP meta-analysis, talk with your MD about whatever contraindication applies, and tick the 10-Point Practitioner Audit listed above to book your appointment. The evidence is clearer than it has ever been, but the practitioner gap remains deep – in 2026 just as in 2019. That’s where the real risk is.
Frequently Asked Questions
Q: Are cupping and Hijama the same?
View Answer
No. Hijama is technically a specific kind of wet cupping involving drawing a small amount of blood through superficial skin scratches, and is the form used in Islamic Prophetic medicine. Cupping is the broad term covering dry cupping, wet cupping (hijama), fire cupping, facial cupping, and moving cupping — none of which (apart from hijama itself) involve breaking the skin.
Q: Is Hijama good for autoimmune disease?
View Answer
Some studies have looked at cupping in rheumatic conditions – the El Hasbani 2021 review in PMC examined cupping in rheumatic diseases and found “variable outcomes.” Hijama is not a stand-alone treatment for autoimmune disease and should never substitute for prescribed disease-modifying therapy. If you have an autoimmune condition, talk to your rheumatologist before adding any complementary practice, and rule out anticoagulant or immunosuppressive interactions before considering wet cupping specifically.
Q: Does cupping help with nerve entrapment?
View Answer
Cupping for nerve entrapment is anecdotally popular but has limited high quality evidence. A 2024 meta-analysis with low back pain applied by extension to some radicular symptoms, but specific nerve entrapment trials are rare. Carpal tunnel syndrome checks off Cleveland Clinic’s list of conditions in which some patients feel relief, but the evidence base is weak.
Q: How is wet cupping different from cupping therapeutically?
View Answer
Wet cupping (hijama) traditionally targets a wider therapeutic window — the Middle Eastern and TCM systems both use it as a method of treatment for migraines, hypertension, and inflammatory medical conditions, on the notion that drawing a small volume of blood removes “heat” or “stagnation” from the localized area. Dry cupping typically applies more to musculoskeletal complaints, sports recovery, and general relaxation, and is the traditional method most associated with the Chinese TCM cupping technique. Current peer-reviewed evidence is strongest for both forms in chronic pain conditions — including chronic low back pain and chronic non-specific pain — and weaker for either one’s broader claims. Hijama cupping increasingly appears in clinical research alongside acupuncture combined with cupping therapy as an integrative-medicine option.
Q: Should I eat before a Hijama session?
View Answer
Practitioner suggestion is a light meal 2-3 hours in advance. Most old sources do not recommend a hot meal immediately before hand and many recommend a chicken fed fast in accordance with Qingming traditions. Only pragmatic worry is a shadowy concern with faintness – entering a wet cupping session on an empty stomach if prone to blood draws vasovagal syncope is a concern.
Q: Can cupping therapy cause blood clots?
View Answer
Unlike blood draws, cupping is not known to cause blood clots but Cleveland Clinic does recommend avoiding cupping in patients with pre-existing clotting disorder such as DVT history or stroke history. The markings are not true ecchymoses that traumatize muscle fibers – they are local capillary rupture near the skin. Consult your physician before cupping if you’re on an anticoagulant such as Warfarin
About This Guide
This hijama vs cupping guide consolidates the 2024-2025 peer-reviewed cupping literature the Cleveland Clinic and AJIC published clinical reviews along with the lived TCM cupping tradition that Tong Ren Tang has carried forward since 1669. Approved by the Tong Ren Tang TCM heritage team – its lineage of 350 years has practiced both dry cupping in Chinese tradition and provides context for hijama wet cupping traditions documented in Islamic Prophetic medicine.
References & Sources
- Cupping (Hijama) in Rheumatic Diseases: The Evidence — El Hasbani et al., 2021, PMC (NIH)
- The effectiveness of cupping therapy on low back pain: A systematic review and meta-analysis — 2024, PubMed
- Cupping for Patients With Chronic Pain: A Systematic Review and Meta-Analysis — Cramer et al., 2020, The Journal of Pain
- The effect of wet cupping therapy on the clinical symptoms of adult asthma — 2024, PMC (NIH)
- Effects of cupping therapy on chronic musculoskeletal pain — 2025, PMC (NIH)
- Cupping Therapy — Furhad & Bokhari, StatPearls, NCBI Bookshelf, 2023
- Practice of cupping (Hijama) and the risk of bloodborne infections — Rehman et al., 2014, American Journal of Infection Control
- Cupping Therapy: Definition, Types & Benefits — Cleveland Clinic Health Library
- The Efficacy of Dry Cupping Compared to Placebo — 2025, Journal of Orthopaedic & Sports Physical Therapy
- Call for Hijama therapy regulation — BBC News, 2014
- The Ridiculous And Possibly Harmful Practice Of Cupping — Steven Salzberg, Forbes, 2019
- Phelps Dives Deeper into the Pseudoscience of Cupping — Skeptical Inquirer
Related Articles
- traditional chinese medicine cupping fundamentals – TCM technique and meridian theory
- acupuncture vs cupping therapy – when to use which complementary practice
- Chinese herbal medicine basics – the Tong Ren Tang formulary tradition
- TCM treatments for chronic back pain – beyond cupping
- TCM perspectives on migraine – herbal, acupuncture, and cupping options
- History of Tong Ren Tang – within 350 years the imperial-class chinese medicine