Get in Touch with Tongren Tang Gulf
![PCOS Treatment A Complete Guide to Your Options [2026]](https://tongrentang.ae/wp-content/uploads/2026/04/PCOS-Treatment-A-Complete-Guide-to-Your-Options-2026.webp)
PCOS Treatment Options: An Evidence-Based Guide to Managing Polycystic Ovary Syndrome
| PCOS at a Glance | |
|---|---|
| Condition | Polycystic Ovary Syndrome (PCOS) |
| Prevalence | 10–13% of reproductive-age women (WHO, 2026) |
| Diagnosis | Rotterdam criteria: 2 of 3 features |
| First-line | Lifestyle modification |
| Key medications | Metformin, OCP, Letrozole, Spironolactone |
| Timeline | 3–6 months for noticeable improvement |
| Cure | No — but symptoms are manageable with the right approach |
If you’ve been diagnosed with polycystic ovary syndrome – or think you might have it – you might be overwhelmed by conflicting nutritional advice, supplement suggestions and lifestyle hacks. In reality, treatment is about tailoring your approach to your own body and goals (whether that’s dealing with acne, improving fertility or reducing your diabetes risk). Below you’ll find an overview of all the main treatment options, underpinned by clinical studies, so you can speak more intelligently with your doctor.
What PCOS Actually Is — and Why It Needs More Than One Treatment
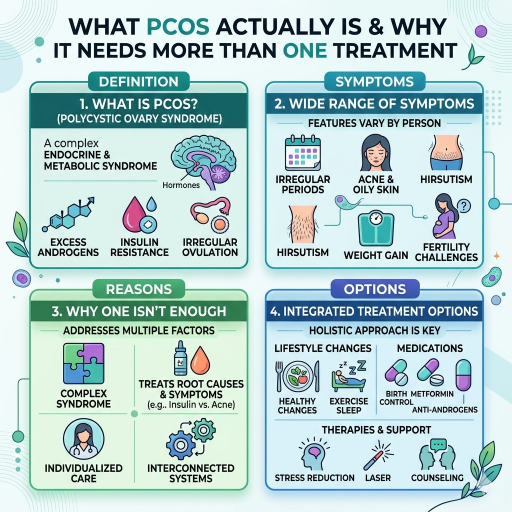
Polycystic ovary syndrome (PCOS) is a hormonal and metabolic disorder affecting 10-13% of women of reproductive age globally (World Health Organization, 2026 info sheet). It is one of the most common endocrine disorders. Yet around 70% of women with PCOS are undiagnosed.
The prevalence of PCOS in the Middle East and North Africa (MENA) region is estimated to be 11.9%, and has been increasing over recent decades (Nahla et al., 2022 systematic review in Nature Scientific Reports). Contributing factors for the high and increasing prevalence of PCOS in Dubai and the UAE may include dietary fat intake, 25 hydroxyvitamin D deficiency, and genetic factors.
The Four PCOS Phenotypes
Why do some women with PCOS not fit a clinical profile? Based on which of the Rotterdam criteria are present, researchers have identified four phenotypes:
- Phenotype A (Classic): High androgens + irregular ovulation + polycystic ovaries on ultrasound
- Phenotype B (Classic without PCO): High androgens + irregular ovulation, normal ovaries
- Phenotype C (Ovulatory): High androgens + polycystic ovaries, but regular cycles
- Phenotype D (Non-hyperandrogenic): Irregular ovulation + polycystic ovaries, normal androgen levels
Your best treatment option depends on your phenotypic presentation. For example, you may not require any anti-androgen medication if you are a Phenotype D woman.
The Insulin-Androgen Loop
In PCOS the ovaries produce too many androgens (male sex hormones like testosterone) through a circuitous process wherein hyperinsulinemia signals the ovaries to produce excess androgens. Such excess androgens cause a failure of ovulation which in turn perpetuates the hormonal and metabolic imbalance – thereby accelerating all the underlying pathways. Effective treatment therefore involves overthrowing this vicious cycle.
💡 Common Misconception: “PCOS Means You Have Cysts”
Polycystic ovary syndrome is a misnomer since Ovarian cysts are not necessary for diagnosis. Those cysts seen on ultrasound reports are tufted out follicles that are present during the peri-ovulatory period, and Endocrine Society states that one can have PCOS in the absence of cysts on the ovaries and vice versa.
Global Prevalence
1 in 8 to 1 in 10 women affected, but 70% remain undiagnosed
How PCOS Is Diagnosed — Tests Your Doctor Will Run

Diagnosing PCOS depends on the Internationally Accepted Rotterdam criteria which states that two of three features should be present:
- Irregular/absent ovulation (irregular or absent menses)
- Biochemical or clinical symptoms of excessive androgen levels (acne, increased hair growth, or raised testosterone levels)
- Multiple cysts on the ovaries (anyone with 12+ follicles or enlargement of ovaries will be diagnosed as Polycystic ovaries)
Other conditions that mimic PCOS (e.g. Hyperprolactinemia, (tumors of the pituitary gland) or Hyperthyroidism should be confirmed first before diagnosis.)
Blood Tests for PCOS
| Test | What It Measures | Why It Matters |
|---|---|---|
| LH & FSH | Luteinizing hormone, follicle-stimulating hormone | LH:FSH ratio often elevated in PCOS |
| Total & Free Testosterone | Androgen levels | Confirms hyperandrogenism |
| DHEA-S | Adrenal androgen | Rules out adrenal source |
| Fasting Insulin | Insulin resistance | Drives treatment decisions (metformin, lifestyle) |
| HbA1C | Average blood sugar (3 months) | Screens for pre-diabetes or diabetes |
| Lipid Panel | Cholesterol, triglycerides | Cardiovascular risk assessment |
| TSH | Thyroid function | Rules out thyroid disorder |
When to see a doctor: Less than 8 menstrual cycles per year, persistent acne unresponsive to topical treatment, unknown hair growth on the face or body, trouble conceiving after one year.
Medical Treatments for PCOS — What Your Doctor May Prescribe
There is no “silver bullet” medication that treats every symptom of PCOS. The best meds for you depend on what concerns you most — irregular periods, fertility, excess hair growth, or metabolic risks. Here is how the main options compare (always discuss with your doctor to find the best options for your personal needs) …
Medication Comparison
| Medication | Mechanism | Best For | Timeline | Key Side Effects |
|---|---|---|---|---|
| Metformin (500–2000 mg/day) | Reduces insulin resistance, lowers hepatic glucose output | Insulin resistance, metabolic PCOS, weight management | 3–6 months | GI upset (nausea, diarrhea); reduced with extended-release |
| Combined OCP | Suppresses ovarian androgen production, regulates cycles | Irregular periods, acne, hirsutism (not trying to conceive) | 1–3 months for cycle regulation | Blood clot risk, mood changes, headaches |
| Spironolactone (25–200 mg/day) | Blocks androgen receptors | Hirsutism, hormonal acne, hair thinning | 3–6 months for visible results | Frequent urination, dizziness; teratogenic (requires birth control) |
| Letrozole (2.5–7.5 mg/day, cyclical) | Aromatase inhibitor; stimulates ovulation | Fertility (first-line ovulation induction) | 1–3 cycles | Hot flashes, fatigue, headache |
| Clomiphene (50–150 mg/day, cyclical) | Selective estrogen receptor modulator; triggers ovulation | Fertility (older standard, now second-line) | 1–6 cycles | Hot flashes, bloating, multiple pregnancy risk (~8%) |
| GLP-1 Agonists (e.g., liraglutide, semaglutide) | Incretin-based; reduces appetite, improves insulin sensitivity | PCOS with obesity and insulin resistance (emerging) | 12–16 weeks for metabolic changes | Nausea, vomiting; must stop before conception |
What the Clinical Data Shows
If the main concern is helping you get pregnant, the evidence is unequivocal: letrozole is clearly better than clomiphene. A critical NEJM trial showed that in women with PCOS, letrozole increased ovulation (relative risk 1.20) and pregnancy rates (relative risk 1.44) more than clomiphene. Consequently, most current guidelines now recommend letrozole for ovulation induction.
If the main concern is managing metabolic concerns, metformin is still the dominant medication, but this is changing (see our Glucagon-like peptide-1 agonists section). According to Truveta, prescriptions for GLP-1 agonists like semaglutide among women with PCOS rose 7-fold from 2.4% to 17.6% between 2021-2025. While GLP-1 medications look promising for weight loss and blood sugar control in PCOS, they are still only an emerging treatment, and not yet widely adopted.
Choosing the Right Medication: A Goal-Based Framework
📐 Decision Framework
- Goal: Regulate periods + reduce acne/hair growth Combination OCP (+ spironolactone if hair growth is severe)
- Goal: Want to conceive? Letrozole first, add metformin if insulin resistant
- Goal: Reduce insulin resistance + improve metabolic health? Metformin (+ lifestyle modifications as foundation)
- Goal: Lose weight + insulin resistance? consult your endocrinologist about GLP-1 receptor agonists
For a Traditional Chinese Medicine-based approach that works in tandem with standard treatment, check out our PCOS treatment protocol, which employs acupuncture and herbal medicines to support ovarian activity and hormonal status.
Lifestyle Changes That Make a Measurable Difference

Every major guideline from recent years recommends lifestyle modification as first-line therapy—before starting medications. And that makes sense: even moderate changes can produce significant results.
The 5% Rule
Both the World Health Organization and StatPearls clinical guidelines recommend that reducing weight by just 5% can result in clinically significant improvements in ovulation, menstruation, androgen levels, and insulin sensitivity. For an individual weighing 80 kg, this means just a 4kg weight loss—which is not dramatic, and indeed, some women estimate that they need to lose much more.
Common misconception: “I Need to Lose 20 kg to See Results”
Clinical research shows regularly that a 5-10% reduction in body weight is linked to clinical improvements in PCOS. Trying to reach excessive target weights may induce hormonal worsening through drastic caloric restriction and undue psychological stress. Small, consistent improvements tend to make the biggest difference.
Diet Approaches with Evidence
No single food plan has proven to be more effective for PCOS in the literature, but three patterns of eating have demonstrated benefit across trials:
- Mediterranean diet: Emphasizes nuts, cereals, fresh vegetables, olive oil, and fish. Has been associated with decreased inflammatory markers and improved insulin sensitivity in women with PCOS.
- Low-glycemic-index diet: Focus on choosing foods that release blood glucose slowly. Has been shown to improve insulin control and menstruation in women with polycystic ovary syndrome.
- Anti-inflammatory diet: highlights omega-3, leafy greens, berries, and nuts, while avoiding processed food and refined sugar. Targets the ongoing, low-grade inflammation that characterizes PCOS.
What they have in common: avoiding refined carbohydrate, and increasing fiber, while adopting a healthy fats diet. Choose the diet you can stick with long-term—a recurring theme in any PCOS patient forum.
Exercise Protocol
Evidence indicates that PCOS optimal lifestyle treatment involves:
- Resistance training (weights and resistance bands): three times a week. Has a unique androgen-lowering effect that cardio does not provide and improves insulin sensitivity in muscle tissue.
- Moderate-intensity cardio (brisk walking, cycling, swimming): minimum of 150 mins a week (roughly five 30-minute sessions). Improves cardiovascular health and weight loss.
No need to train like an athlete. Consistency over intensity: the Reddit PCOS community frequently notes that regular “half an hour a day” of movement was life-changing.
Sleep and Stress
Cortisol (the stress hormone): directly impairs insulin sensitivity and androgen production. Target factors impairing sleep quality: ensure seven to nine hours of sleep daily, and implement stress-reduction strategies such as meditation, walking, or other favored methods that reduce baseline cortisol levels. Sleep disturbances are prevalent in PCOS, often related to higher incidences of sleep apnea.
For those concurrently addressing weight-related issues, our obesity program combines Lifestyle interventions with Traditional Chinese Medicine (TCM). If sleep disturbances are a concern, consider our acupuncture-driven insomnia Program.
✔ Weekly PCOS Lifestyle Checklist
- 3 resistance training sessions completed
- 150 minutes of moderate cardio logged
- Meals followed a low-GI or Mediterranean pattern
- 7–9 hours of sleep most nights
- At least one intentional stress-reduction practice
Natural Therapies, Supplements, and Symptom Management
Supplements are one of the most searched-for topics in regards to PCOS management. Evidence continues to develop—yet, it’s wise to differentiate established clinical trial data from emerging evidence.
Supplement Evidence Table
| Supplement | Evidence Level | Typical Dose | What It Targets |
|---|---|---|---|
| Myo-Inositol + D-Chiro-Inositol | Strong (conditional recommendation in 2023 guidelines) | 4000 mg myo + 100 mg D-chiro (40:1 ratio) | Insulin signaling, ovulation, egg quality |
| Vitamin D | Moderate (if deficient) | 1000–4000 IU/day based on blood levels | Insulin resistance, menstrual regularity, mood |
| Berberine | Moderate | 500 mg 2–3x/day | Insulin resistance, lipid profile (comparable to metformin in some trials) |
| NAC (N-Acetyl Cysteine) | Preliminary | 600–1800 mg/day | Antioxidant, may improve ovulation and insulin levels |
| Omega-3 Fatty Acids | Preliminary | 1000–3000 mg/day (EPA + DHA) | Inflammation, triglycerides, mood |
The most well-supported supplement is inositol. A 2024 systematic review published in the Journal of Clinical Endocrinology & Metabolism (JCEM) assessed inositol’s benefits for PCOS, contributing to the new international PCOS guidelines which include a conditional endorsement of the supplement.
Conversely, the Society of Obstetricians and Gynaecologists of Canada (SOGC) notes “a lack of evidence for specific dosing guidance” for many supplements. Bottom line: supplementation such as inositol may be used as a complement, but not a substitute, for clinical treatment and proven health strategies.
⚠️ Supplement Quality Warning
Supplements are not subject to the same quality and safety regulations as pharmaceuticals. Quality can vary widely between brands. Check for third-party testing rankings (USP, NSF, ConsumerLab), and consult your health care practitioner before incorporating new supplement into your regimen, especially if you already take prescription medications.
Managing Cosmetic Symptoms
Many symptoms of PCOS are visible and can be anxiety-provoking; here are the solutions our patients have benefited from:
- Acne: Topical retinoids and benzoyl peroxide for mild to moderate cases, or hormonal contraceptives or spironolactone for more severe hormonal acne. Results in three to four months.
- Excess hair: Laser hair removal (best for dark hair on light skin), electrolysis (suitable for all skin and hair colors), or eflornithine cream (limits facial hair growth). Hormonal therapies target the underlying hormonal imbalance.
- Determining the causes of hair loss/thinning/ excess hair: Spironolactone, minoxidil (topical) or a combination. Results seen in 6-12 months. Balancing insulin resistance and androgen excess will support regrowth.
In traditional Chinese medicine (TCM), further options are available for treating symptoms of the syndrome. Research has looked at ovarian effects of acupuncture, and managing ovarian function. Find out more about PCOS acupuncture treatment at our clinic. If herbal medicine is preferable, our Chinese herbal medicine guide can tell you how formulas are tailored to your individual presentation. Our online PCOS pattern assessment also helps determine your TCM constitution type.
PCOS and Fertility — Treatment When You Want to Conceive

Many women worry most about how polycystic ovary syndrome affects trying for a family. It won’t affect you having children. Despite being the commonest cause of ovulatory infertility, most women with PCOS can conceive with support.
💡 Misconception: “PCOS Means You Can’t Have Children”
PCOS makes conception harder — not impossible. With ovulation-inducing medication, the majority of women with PCOS ovulate successfully, and many conceive within 3–6 cycles of treatment.
The Treatment Escalation Path
Fertility treatment for PCOS typically follows a step-by-step escalation:
- Lifestyle changes (3-6 months): Weight reduction, exercise and diet may induce ovulation without medication.
- Letrozole (first line medication): The NEJM study proved this to be a more successful ovulation inducer than clomiphene (increase live birth rate). Ovulation relative risk: 1.20. Pregnancy relative risk: 1.44.
- Clomiphene + Metformin (second line): If letrozole is unsuccessful, the addition of metformin to improve insulin function and ovary response.
- Gonadotrophins/injective hormones. Effective but require close monitoring of ovarian response and use when other treatments are unsuccessful.
- IVF/in vitro fertilisation. Usually the last step in fertility treatment. Women with PCOS respond well to ovarian stimulation but require specialist protocol management.
Women should be regularly monitored throughout the fertility procedure, given the increased risk of diabetes, pre-eclampsia and preterm delivery in women with PCOS who conceive.
Acupuncture is being sought alongside fertility medication in PCOS. Our IVF acupuncture support program is designed to work during their IVF protocols. Read about other ways TCM supports PCOS pregnancy in our PCOS treatment details.
Long-Term Health Risks and When to See a Specialist

PCOS isn’t just about conceiving, in the meantime you face long term health problems. Ongoing clinical monitoring is necessary. The World Health Organization advises this focus as long term health concerns for women with PCOS:
- Type 2 diabetes: risk is much more higher in women with PCOS, many developed it through persistent insulin resistance. Up to 40% of women develop it before menopause.
- Cardiovascular disease: health problems already measured from early age include high cholesterol, blood pressure and triglycerides.
- Endometrial cancer: irregular periods mean that the lining of the womb has a greater exposure to oestrogen than the other woman’s, with a consequent increased risk of developing endometrial carcinoma.
- Obstructive sleep apnea: 5-10 times more common in PCOS women, especially those with higher BMI.
- Depression and anxiety: changes in hormones, negative body image and problems conceiving may all be factors. Screening for depression and anxiety should be a standard part of polycystic ovary syndrome care.
Annual Screening Checklist
✔ Recommended Annual Tests for Women with PCOS
- Fasting glucose and HbA1C (diabetes screening)
- Lipid panel (cardiovascular risk)
- Blood pressure check
- Mental health screening (PHQ-9 for depression, GAD-7 for anxiety)
- Pelvic ultrasound if periods are absent or very irregular
- If you have symptoms of apnea such as snoring or excessive daytime fatigue you should be assessed for sleep problems.
When to Escalate Care
Consult an endocrinologist or infertility specialist if: six months of a symptom not responding to first-line treatment; planning pregnancy without ovulation while on medication; development of signs of cardiovascular disease or diabetes; or severe depression or anxiety that impair functioning.
If you are considering treatments for risk of diabetes in conjunction with PCOS, our diabetes care with traditional Chinese medicine program will consider blood glucose regulation with acupuncture and Chinese herbal medicine. If you are approaching menopause with concomitant PCOS, hormonal changes will require different management — we encourage you to see our page on menopause care.
Frequently Asked Questions About PCOS Treatment

Can PCOS be cured permanently?
View Answer
There is no current cure for polycystic ovary syndrome: it is a chronic condition related to genetic and metabolic factors that cannot be eradicated. The condition can be managed through life style changes, medications and regular assessment. Many women report a significant symptomatic improvement and some enter remission- especially after significant weight loss or hormonal compensation.
What is the most effective treatment for PCOS?
View Answer
There is no single available treatment because symptoms of polycystic ovary syndrome are different in each woman. Metabolic abnormalities are best treated with lifestyle and metformin. Fertility treatment is best addressed with the medication letrozole. Hirsutism and acne are best treated with combined oral contraceptive pills and a medication spironolactone. Many women use multiple treatments. Traditional Chinese medicine including acupuncture and herbal preparations are also used as adjunct therapies depending on symptoms- learn more about Traditional Chinese Medicine for PCOS.
How long does PCOS treatment take?
View Answer
Treatments for polycystic ovary syndrome generally will begin show small improvements over 3-6 months. Metformin and life style therapies show results within three months. Anti-hormones such as spironolactone show results in 3-6 months. Fertility treatments are individualized but most take 1-3 cycles.
Can I get pregnant if I have PCOS?
View Answer
Almost certainly yes. While polycystic ovary syndrome accounts for the largest number of episodes of ovulatory infertility it is possible to conceive with appropriate treatments. Ovulation medications such as letrozole have significantly higher success rates than previous medications such as clomiphene. Other treatments are gonadotropins with injections and in-vitro fertilization. Many women conceive on their own with or without additional therapeutic interventions- especially with modest weight reduction.
Is PCOS treatment lifelong?
View Answer
Ongoing and changing. In your twenties your focus will most likely be on acne and hormonal birth control use and in your thirties probably on conceiving and in your forties monitoring for metabolic complications. Your diet, exercise and sleep need to be balanced and healthy at all stages of life.
What can trigger a PCOS flare-up?
View Answer
What can worsen the symptoms of PCOS after the patient has been stable for a few years. Specific things that can bring about worsened PCOS symptoms include:
Large weight increase leads to increased insulin resistance which drives androgen excess and anovulation. Prolonged stress leads to increased cortisol which worsens the hormonal disruption. Poor sleep (fewer than 6 continuous hours) worsens insulin resistance and affects hormonal appetite regulation. Discontinuing medication (coming off birth control or metformin) may cause symptoms to recur. Dietary change towards high refined sugar high processed food diet high insulin release. Major life/position changes – relocation, changing jobs, relationship/ relationship difficulty- can lead to flaring through the stress/cortisol axis. Consistency in lifestyle practices is best protection from PCOS recurrence.
Ready to Take the Next Step?
Our practitioners who hold the DHA-license develop a personalized PCOS therapy to complement your existing healthcare.
About This Guide
This PCOS treatment guide was conceived and produced by Tong Ren Tang, a TCM heritage institution over 350 years old, now providing Dubai access through DHA-licensed practitioners. While we prioritize TCM-based PCOS management in our clinical practice, we believe patients are empowered through understanding all available treatment options. This article does not promote any specific treatment or concept and declares no financial support from pharmaceutical companies. All conclusive evidence in this publication is backed by references listed below.
References & Sources
- World Health Organization. Polycystic Ovary Syndrome. Fact Sheet (January 2026). who.int
- Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus Clomiphene for Infertility in the Polycystic Ovary Syndrome. New England Journal of Medicine. nejm.org
- Fitz V, Graca S, Engmann L, Boyle J. Inositol for Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Journal of Clinical Endocrinology & Metabolism. 2024;109(6):1630. academic.oup.com
- Rasquin Leon LI, Mayrin JV. Polycystic Ovarian Syndrome. StatPearls [Internet]. ncbi.nlm.nih.gov
- Naz MSG, et al. The Burden of Polycystic Ovary Syndrome in the Middle East and North Africa Region. Nature Scientific Reports. 2022. nature.com
- Truveta Research. Rising Use of GLP-1 Medications Among Women with PCOS. 2025. truveta.com
- Endocrine Society. Fact or Fiction: PCOS Myths Debunked. endocrine.org