Get in Touch with Tongren Tang Gulf
Acupuncture and dry needling seem to be the same thing when it comes from your point of view sitting at the table: a clinician presses a tiny metal needle into an inflamed point, and you wait for the effects to happen. But look deeper, and you will notice two distinct medical histories, two distinct licensing agencies, and two different sets of rules on what your insurance coverage could be in 2026. Here is a side-by-side guide to help you decide which one belongs on your treatment plan, with citations from the National Institutes of Health, the Centers for Medicare & Medicaid Services, and the American Physical Therapy Association.
Quick Comparison Snapshot
| Origin | Acupuncture — Traditional Chinese Medicine, ~2,500 years | Dry needling — Western anatomy, since the 1940s |
| Theory | Energy flow (Qi) along meridian lines | Neuromuscular trigger points and motor endplates |
| Practitioner | Licensed acupuncturist (L.Ac.), ACAOM-accredited training | Physical therapist with state-approved dry needling certification |
| Typical Needle Depth | 5–25 mm | 10–50+ mm (depending on the muscle belly) |
| Retention Time | 20–40 minutes | Seconds to a few minutes (often in-and-out) |
| Medicare 2026 Coverage | Yes — chronic low back pain only, up to 20 visits/year | No — not covered for any condition |
Here’s the briefest prudent summary: same monofilament needle, two medicines – separated by 2,400 years and one philosophy. Next we’ll explore what each modality is, where the science actually lines up with the marketing, and how to choose between them for back pain, sciatica, TMJ or a frozen shoulder.
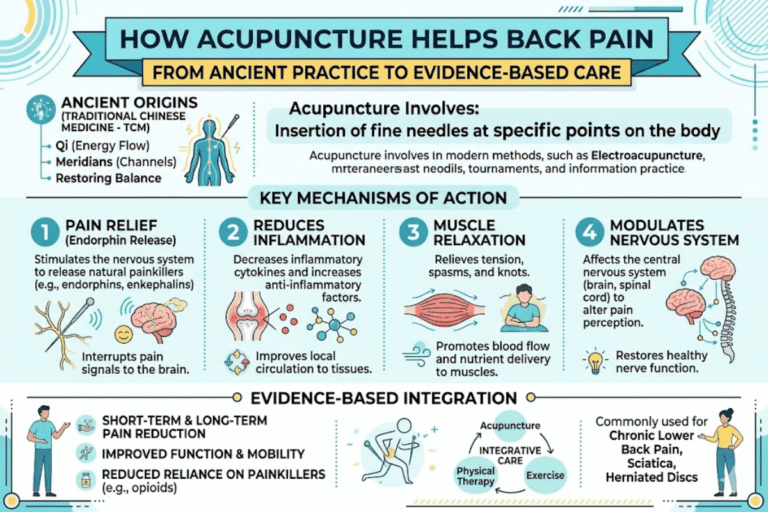
What Is Acupuncture? A 2,500-Year-Old TCM Practice

Acupuncture is a treatment that involves the insertion of very thin, sterile needles into selected points on the body. It has been in practice for at least 2,500 years and is used in 103 of the 129 participating World Health Organization member nations, according to the U.S. National Center for Complementary and Integrative Health. The percentage of the adult US population (2.2%) who reported using acupuncture increased more than two-fold between 2002 and 2022 (1.0%) (National Health Interview Survey).
Classical theory has its roots in the approaches of Traditional Chinese medicine: acupuncturists needled along the meridians which (in theory) are associated with the various organ systems and with the pathway of Qi, or energy. When this energy path is interrupted or in imbalance, the practitioner believed disease or pain to result; the practice of needling along the meridians presumably was intended to produce a balancing response and also to stimulate the body to activate its healing mechanisms. By contrast, many accounts in the Western literature describe this same intervention with the help of different concepts: needling, according to some authors, “stimulation[s] nerve endings, muscles, and connective tissue, with a resulting effect(s) on central pain processing”, described in the NCCIH press release as “effects on nervous system function” seen in imaging studies.
Regardless of which framework you lean toward, the U.S. practitioner standard is uniform. A licensed acupuncturist (L.Ac.) usually holds a master’s or doctoral degree from an ACAOM-accredited program, and is certified by passing the NCCAOM national board exam — about 3,000 hours of training. In Western medicine, the same insertions are often described as locally increasing blood flow, stimulating connective tissue, and modulating nerve signaling. The U.S. Food and Drug Administration regulates acupuncture needles as medical devices and requires that they be sterile and labeled for single use.
What Is Dry Needling? A Modern Western Therapy

Dry needling appears similar on the surface — a clinician inserts a thin monofilament needle through the skin — yet the framework around it is anchored in Western anatomy. Nothing is injected (hence “dry”); the needle itself is the treatment. The target is a myofascial trigger point: a hyperirritable nodule inside a taut band of skeletal muscle, palpable as a knot, which often produces referred pain elsewhere in the body when pressed.
Lineage originates with Dr. Janet Travell, who first mapped out trigger points in the 1940s, and became President Kennedy’s personal physician. Travell was teamed up with Dr. David Simons, and the textbook they co-authored is the defining source for the field. A second generation of providers was driven in the 1970s by Dr. C. Chan Gunn, who pioneered Intramuscular Stimulation (IMS); this approach uses needles to activate motor points along peripheral nerves, not classical trigger points alone. Today, dry needling practitioners are generally comfortable drawing from both lineages.
According to the American Physical Therapy Association, dry needling is most often performed by physical therapists who have completed additional state-approved training post-licensure — typically a 27–54 hour course, depending on jurisdiction. Its purpose within physical therapy is to reduce muscle pain and tightness and improve range of motion, as part of a broader plan that includes hands-on therapy and exercise. The 2021 clinical practice guideline by Gattie, Cleland, and Snodgrass in The Journal of Orthopaedic & Sports Physical Therapy found dry needling effective for several musculoskeletal conditions when paired with active therapy.
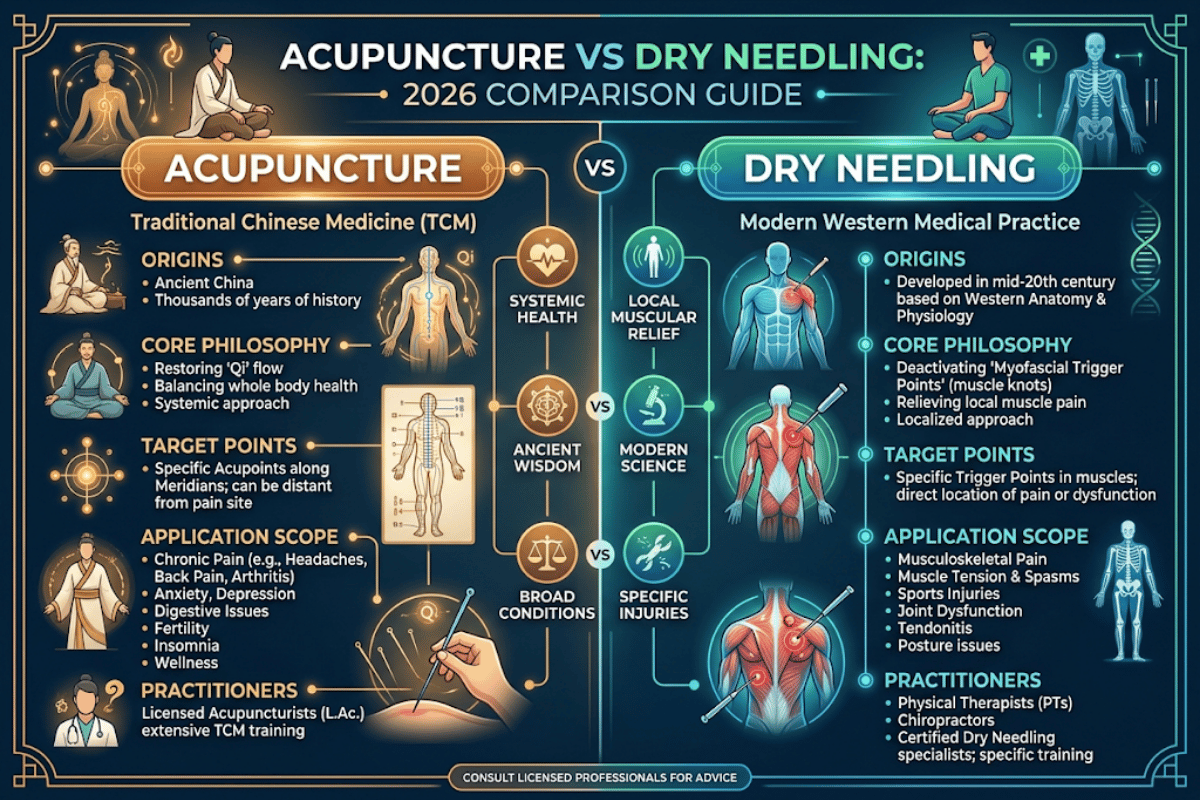
Acupuncture vs Dry Needling: 7 Real Differences

If you only take away one thing, take this: same monofilament needle, two different medicines. The reasons dry needling and acupuncture diverge run from underlying theory to billing code; a side-by-side comparison is below.
| Dimension | Acupuncture | Dry Needling |
|---|---|---|
| 1. Theoretical framework | TCM — meridians, Qi, pattern-based diagnosis | Western anatomy — trigger points, motor endplates, neuromuscular dysfunction |
| 2. Where the needle goes | Acupuncture points along meridian lines, often distal to the painful area | Directly into the painful trigger point or motor point of the involved muscle |
| 3. Typical depth | 5–25 mm | 10–50+ mm into the muscle belly |
| 4. Time on the table | Needles retained 20–40 minutes | In-and-out, or held for seconds to a few minutes; often a “sparrow pecking” technique |
| 5. Practitioner | Licensed acupuncturist (L.Ac.) — ACAOM master’s + NCCAOM exam, ~3,000 hours | Physical therapist + state-approved dry needling course (27–54 hours typical) |
| 6. Regulatory status | Licensed in most U.S. states; needles are FDA-regulated single-use medical devices | Permitted in most states for PTs; a few jurisdictions restrict or remain silent (per APTA April 2026 map) |
| 7. Medicare 2026 coverage | Covered for chronic low back pain (cLBP) under CMS NCD 30.3.3 | Not covered for any condition |
📑 Regulatory Note
The one detail that every single patient guide on the subject omits: under Medicare rules, CMS considers them both a form of acupuncture. The 2020 National Coverage Determination reads “All types of acupuncture including dry needling for any condition other than cLBP are non-covered by Medicare.” This means that Medicare considers the two interventions the same family; just one branch is billed for cLBP and the other is not recognized by the federal regulator at all.
Which One for Your Condition? Back Pain, Sciatica, TMJ, and More

Asking about differences in “which is better” generally accomplishes little. What’s more appropriate is “which intervention is better for the pain that I have now?” Below is a summation of where the strongest evidence currently points for most conditions that patients inquire about, citing primarily the NCCIH, and The 2017 American College of Physicians clinical practice guideline.
| Condition | Stronger Evidence For | Why |
|---|---|---|
| Chronic low back pain | Acupuncture | Recommended as first-line nondrug therapy by the 2017 ACP guideline; covered by Medicare since 2020 |
| Acute neck pain or stiffness | Either — depends on cause | NCCIH 2018 review (8,003 participants) supports acupuncture; JOSPT 2021 supports dry needling for muscular neck pain |
| Sciatica | Acupuncture (with caveats) | 2015 evidence reviews suggest benefit; quality of research is mixed |
| TMJ / jaw pain | Either, often combined | Both target the masseter and surrounding muscles; pick by practitioner expertise and access |
| Frozen shoulder | Dry needling (paired with PT) | Capsular and rotator-cuff restriction usually needs hands-on mobility work that PTs already deliver |
| Tennis or golfer’s elbow | Dry needling | Localized tendinopathy responds to direct trigger-point work; combine with eccentric loading |
| Migraine prevention | Acupuncture | 2016 review of 22 studies (~5,000 people) showed reduced migraine frequency vs. no treatment |
| Fibromyalgia | Acupuncture | 2019 review of 12 studies (824 participants) found acupuncture better than sham |
| Knee osteoarthritis | Acupuncture | Conditionally recommended in the 2019 American College of Rheumatology / Arthritis Foundation guideline |
| Sports recovery, post-workout knots | Dry needling | Designed for localized myofascial pain; effects often felt within 1–3 sessions |
If your pain is limited to one specific muscle, just the exact one you can find on your own, dry needling will have the better track record. If your pain presents in a broader fashion, is accompanied by sleep or stress issues, or happens inside one of the conditions where the ACP, NCCIH, or American College of Rheumatology has published a guideline (low back, knee osteoarthritis, migraine, fibromyalgia), licensed acupuncture care has a more substantial evidence base.
What the Evidence Says: Effectiveness Comparison

Both interventions hold moderate-level evidence for several conditions, but they are constructed differently in the literature. Acupuncture has a longer trail of high level evidence – it has been studied for centuries, and the Cochrane and NCCIH funded research has been pooling it for decades.
What’s more effective, dry needling or acupuncture?
Honest answer: they have not been directly compared head-to-head in a high-quality systematic review for most conditions. What we do have:
- A 2018 NCCIH-summarized review of a dozen studies, including 8,003 subjects, finds that acupuncture appears more effective than doing nothing for back and neck pain; the effect size is similar to that known from nonsteroidal anti-inflammatory drugs.
- Vickers et al. (2018) published an individual-patient-data meta-analysis in The Journal of Pain including 20 studies (6,376 subjects) demonstrating acupuncture’s pain-relieving effects persisted for up to a year after the last treatment.
- The 2021 JOSPT clinical practice guideline (Gattie, Cleland, Snodgrass) states dry needling effectively reduces pain and improves function for neck and shoulder pain and lower back pain when combined with active therapy.
- A 2019 PMC analysis (PMC6598484) finds that for each modality the bottom line is that deeper needle insertion produces more pain relief than superficial needling — a reminder that depth and technique matter at least as much as the brand name on the door.
One nuance the marketing often leaves out: NCCIH mentions that in numerous studies the difference between acupuncture and no treatment was greater than the difference between acupuncture and sham acupuncture. This indicates a sizable portion of the benefit may originate from non-specific effects–the practitioner relationship, expectation, and one whole hour of deliberate time attending to your body. That doesn’t make the relief any less real, but it does help explain why outcomes seem to differ so widely from clinic to clinic.
Will It Hurt? Depth, Needle Gauge, and What You’ll Feel
Both treatments use non-coring, filiform, monofilament needles- not the hollow-bore syringe needles we associate with injections and blood draws. Typical gauges range from 0.16 to 0.30mm in diameter, much thinner than a 0.7-0.9mm needle used to draw blood. Patients generally describe feeling a brief pinch when the needle is inserted, then nothing at all.
Does acupuncture or dry needling go deeper?
Dry needling can go deeper, which often becomes distinctly obvious. Classical body acupuncture is usually inserted 5 to 25mm depending on the point and the point itself. Dry needling targets the trigger point inside a muscle belly, which can sit anywhere from 10 to 50 mm below the skin surface in thicker muscles such as the gluteals or quadriceps. Once the needle reaches a tight band, you may experience a sudden, involuntary jump or twitch hit – the local twitch response – followed by a dull ache as the tightness inside the muscle lifts; acupuncture seldom produces this twitch, more commonly you’ll report a heavy, dull sensation called de qi in TCM.
Muscle soreness for 24 to 48 hours afterward is common with dry needling and not often reported with acupuncture, simply because dry needling intentionally provokes a controlled muscle twitch. Bruising can also be more prominent with dry needling for the same reason. Neither sensation should be acute or radiating; be sure to tell your practitioner immediately if it is.
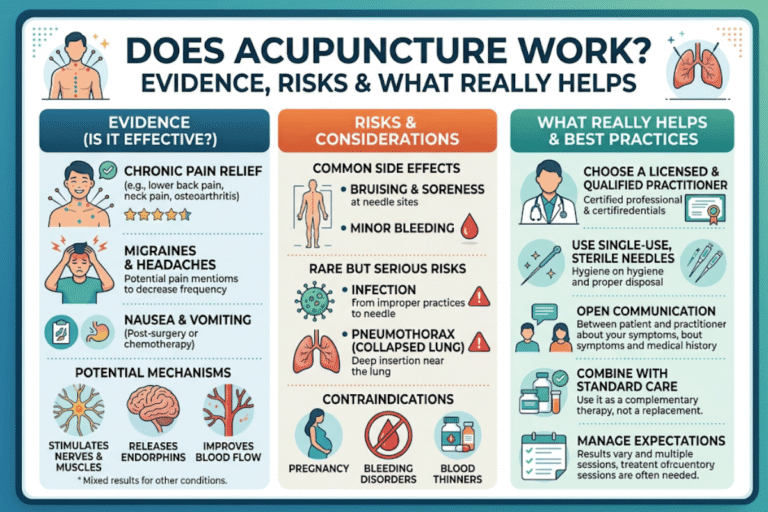
Risks, Side Effects, and Who Should Avoid Either
Both are very safe in the hands of experienced practitioners. The most common adverse effects are light bruising, brief soreness, minor bleeding at the insertion point; all clear up in a day or two. Serious accidents are rare and are most often caused by either unsterile needles or treatment over the lungs.
Who shouldn’t get dry needling treatments?
According to NCCIH and clinical safety reviews, you should consult your provider before either treatment if you:
- ⚠️ Take blood thinners or have a bleeding disorder
- ⚠️ Are pregnant (some practitioners avoid specific points; dry needling is generally not recommended during pregnancy)
- ⚠️ Have an active infection, weakened immune system, or impaired healing
- ⚠️ Use a pacemaker or implanted cardiac device (relevant for electroacupuncture)
- ⚠️ Have an unusual fear of needles — ask for a single-needle test session first
Pneumothorax (collapsed lung) is the most-reported serious adverse event for both modalities when needling in the upper back, shoulder, or chest region. The risk is real but very low — a frequently cited estimate is less than 0.01 per 10,000 acupuncture interventions. A safety study tracking 39 physical therapists across 7,600 dry needling treatments recorded zero pneumothorax cases. Selecting a clinician with explicit training in thoracic-region needling drops the risk further.
Cost, Insurance, and How Many Sessions You’ll Need
Costs in 2026 in most U.S. areas looks about like this:
- Acupuncture: $75-$150 per session at an L.Ac.; initial consultation often $100-$200.
- Dry needling: $40-$100 on top of a typical PT appointment, or $80-$150 standalone.
How your insurance responds is the bigger unknown. Medicare NCD 30.3.3, effective January 21, 2020, covers acupuncture for chronic low back pain only — up to 12 visits in 90 days, with an additional 8 sessions if the first 12 produce improvement, capped at 20 sessions per year. Dry needling is not covered by Medicare for any condition; TRICARE took the same position in 2020. Commercial coverage of acupuncture has grown: an analysis of the Medical Expenditure Panel Survey, summarized by NCCIH, showed the share of acupuncturist visits with any insurance coverage rising from 41.1% in 2010–2011 to 50.2% in 2018–2019. Dry needling commercial coverage remains highly state- and plan-dependent.
How many visits until you know it is working? Acupuncture for a chronic condition generally requires 6 to 12 treatments before judging effect; the ACP guidelines point to roughly that range for low back pain. Dry needling tends to produce a quicker signal — clinicians and patients both report a meaningful difference in 2 to 4 visits, with chronic cases sometimes needing 6 to 8. If you have not noticed a difference after the third or fourth session in either modality, ask your practitioner to reconsider the plan.
How to Decide: The Needle-Choice Framework

Most online comparisons ask “which is better?” That is the wrong question. Below is a 4-question framework patients can answer in two minutes — the answers point to one or the other modality, and not always the same one.
The Needle-Choice Framework
- Where is your pain? A localized muscle knot you can point to with one finger → dry needling. Diffuse, multi-region, or systemic → acupuncture.
- How long has it been there? Acute, post-injury, or under six weeks → dry needling tends to deliver faster relief. Chronic, more than three months → acupuncture has the stronger long-term evidence.
- Are you also dealing with sleep, stress, or digestion issues? Yes → acupuncture, which is built for whole-body pattern treatment. No → either works.
- Is the painful area near the lung, kidney, or major nerve? Yes → favor a licensed acupuncturist with deeper anatomy training, or a PT with explicit thoracic-region dry needling certification.
✔ When acupuncture wins
- Chronic low back pain (Medicare covered)
- Migraine prevention
- Knee osteoarthritis
- Fibromyalgia, sleep, stress overlap
- Pregnancy-related pain (with a trained L.Ac.)
⚠ When dry needling wins
- Localized muscle knots, post-workout
- Tennis or golfer’s elbow
- Frozen shoulder paired with PT
- Acute neck stiffness, trigger-point referred pain
- When you are already in physical therapy
Industry Outlook 2025–2026: Where Needle Therapy Is Heading
Three trends are worth watching if you’re choosing now or treating patients next year.
Demand continues to rise across both markets. Coherent Market Insights projects that the global acupuncture market will be valued at USD 51.66 billion in 2026, rising to USD 79.28 billion by 2033 (compound annual growth rate of around 7.4%). Demand for adult acupuncture use in the U.S. more than doubled between 2002 and 2022 (National Health Interview Survey), with IBISWorld projecting the adult U.S. acupuncturist industry at $825.9 million in 2026.
Regulation is becoming more unified. The Federation of State Boards of Physical Therapy (FSBPT) has continued to refine its dry needling competency framework through 2024 and 2025, moving toward a more standardized post-licensure training requirement. The APTA state-by-state map (April 2026) shows that most states now permit physical therapist dry needling; the holdouts and silent jurisdictions remain the story for any patient near a state line.
Integrative pain care is the new normal. Insurance is making slow progress—commercial acupuncture coverage is over 50% and Medicare enabled cLBP coverage for the first time this year. So if you are considering a 2026 course of treatment—before your first appointment, get a written confirmation from your insurer that your treatment (acupuncture for cLBP or dry needling for musculoskeletal pain) is in-network.
Frequently Asked Questions
Q: Are acupuncture and dry needling the same thing?
View Answer
No, they use the same monofilament needle but the theory, the target, the training and the regulation are different. Acupuncture follows TCM meridian theory, and it is practiced by licensed acupuncturist. Dry needling adheres to Western anatomy and targets myofascial trigger points.
Q: Can I get both acupuncture and dry needling at the same time?
View Answer
Yes- many patients do, and the integrative clinics coordinate them. Most common is dry needling within an acute PT episode addressing one regional pain problem, while the other course presents separately for long term sleep, stress, or chronic pain management. Make sure each provider knows what the other is doing so they complement one another instead of competing.
Q: Is dry needling legal in every U.S. state?
View Answer
No, most states allow PTs to perform dry needling if they are licensed and completed state approved training. A few states do not allow it or have not addressed the question. The APTA has a state by state map, last updated April 2026, on the website (verify current training information before scheduling).
Q: Will my insurance cover acupuncture or dry needling in 2026?
View Answer
Medicare reimburses for acupuncture for chronic low back pain only, capped at 20 visits/year billed under NCD 30.3.3. (Medicare does NOT reimburse for dry needling-any indication). Roughly 50% of commercial policies presently cover acupuncture for at least some diagnoses (Candon et al. JAMA network Open 2022).
Commercial coverage for dry needling is plan by plan; often considered an included modality at the time of a Physical Therapy appointment. Get confirmation of coverage in writing prior to the first appointment.
Q: What are the five forbidden acupuncture points?
View Answer
Classical TCM texts spell out a (very limited) selection of points howling againts for needling another six or so, including LU5 (Chize), ST9 (Renying) and points along the fontanelle in babies, on the gravid abdomen in pregnancy and over the cardiac region. Today’s licensed practitioners are trained to spot them and avoid them; the use of the term ‘five forbidden points’ is merely a useful way of ensuring this basic notion of anatomy-anatomy-anatomy is never forgotten about before needing any patient.
Why a TCM Heritage Brand Is Writing About Dry Needling
Founded in 1669, Tong Ren Tang has been practicing and selling Traditional Chinese Medicine since then, over 188 years as an herbalist appointed to serve the Qing imperial family. Among its lineage is acupuncture ; dry needling is a more recent Western practice that employs some similar tools but within a different context. This is an editorial article – reviewed by our herbalist team for accuracy in TCM but not a substitute for a visit with a licensed acupuncturist or physical therapist to treat your own pain.
References & Sources
- Acupuncture: Effectiveness and Safety — National Center for Complementary and Integrative Health, NIH
- National Coverage Determination 30.3.3 — Acupuncture for Chronic Lower Back Pain — Centers for Medicare & Medicaid Services
- CMS MM11755 Implementation Guidance — Centers for Medicare & Medicaid Services
- Dry Needling in Physical Therapy Practice — American Physical Therapy Association
- State Laws and Regulations Governing Dry Needling Performed by PTs — APTA, April 2026
- Dry Needling Versus Acupuncture (II): AAPAS White Paper 2016 — Fan AY et al., PubMed
- Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis — Vickers et al., The Journal of Pain, 2018
- Pneumothorax as a Complication of Dry Needling Technique — PubMed Central
- Dry Needling in Physical Therapy Practice: Adverse Events — Academy of Orthopaedic Physical Therapy
- Dry Needling Competencies — Federation of State Boards of Physical Therapy
- TRICARE Balks at Covering TENS and Dry Needling — APTA, March 2020
Related Articles
- Traditional Chinese Medicine therapies overview — how acupuncture, herbs, and tui na fit together
- TCM herbs for muscle pain and recovery — classical formulas explained
- Acupuncture for chronic low back pain in 2026 — what Medicare actually covers
- Meridian lines and the flow of energy — a plain-English guide to TCM theory
If a TCM perspective on your pain matters to you — or you simply want to talk through whether acupuncture, dry needling, or something else fits your situation — reach out to a licensed acupuncturist in your area for an initial consultation.