Get in Touch with Tongren Tang Gulf

Quick Specs: Tenosynovitis
| Condition | Tenosynovitis — inflammation of the tendon sheath (synovium) |
| Most Common Type | De Quervain’s tenosynovitis (thumb side of wrist) |
| Prevalence | 0.5% in men, 1.3% in women |
| First-Line Treatment | Rest + splint + NSAIDs (4–6 weeks) |
| Injection Success Rate | 52–90% relief with 1–2 corticosteroid injections |
| Surgical Success | >90% resolution for De Quervain’s release |
| Emergency Red Flag | Suspected infectious tenosynovitis (fever + fusiform swelling + pain on passive extension) |
Topics from repetitive strain to de Quervain’s tenosynovitis for postpartum patients to infectious tenosynovitis emergencies all require different methods of approach – here is a primer that covers them all. We run through each broad range of tenosynovitis, helping you and your physician figure out how to diagnosis it, how to treat it based on real clinical data, and even a simple three step rehabilitation protocol you can print and use at home. And we introduce the 4-6-2 Protocol, a simple decision matrix you can apply with your medical provider to determine when to attempt conservative treatment, then injection and when expert consultation is necessary.
What Is Tenosynovitis — Types, Anatomy, and How It Develops

Tenosynovitis is an inflammation of the synovial membrane, the delicate, fluid-filled layer surrounding your tendons. Every time you move your fingers, bend your wrists, or flex your ankles the sheath allows the tendons to glide and bend smoothly at the joint. When inflamed, thickened, or infected, it loses the ability to produce this frictionless movement, and each type of tenosynovitis causes pain and locking sensation along its course.
It is a distinct condition from Tendonitis, the inflammation of the actual tendon. This in which case develops in the delicate sleeve of the tendon, which is called the synovium. The sheath of the sheath causes the tendons to not glide comfortably anymore and this is the origin of the pain and painful snapping sensation felt during active movement.
Epidemiologic studies have estimated the overall prevalence of De Quervain syndrome (de Quervain’s tenosynovitis) at approximately 0.5% for men and 1.3% among women, with incidence peaks in the fifth and sixth decades of life. Many tendons exist within the body, but most suffer from tendinous or muscular disorder; the hand and wrist are by far the most common sites of pathology.
| Type | Primary Location | Cause | Urgency |
|---|---|---|---|
| De Quervain’s | Thumb side of wrist (1st dorsal compartment — abductor pollicis longus + extensor pollicis brevis) | Repetitive thumb/wrist motion, postpartum lifting | Moderate — respond to conservative care |
| Stenosing (Trigger Finger) | Flexor tendons of fingers (A1 pulley) | Repetitive gripping, diabetes, rheumatoid arthritis | Moderate — injection or release if persistent |
| Infectious (Pyogenic) | Flexor tendon sheath of fingers | Puncture wounds, animal bites, immunocompromised state | Emergency — IV antibiotics + possible surgical drainage |
| Inflammatory (Autoimmune) | Multiple joints (wrist, hand, feet) | Rheumatoid arthritis, lupus, psoriatic arthritis, gout | Chronic — requires systemic treatment (DMARDs) |
📐 Engineering Note — Anatomy Detail
The first dorsal compartment of the wrist is the passageway of the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB) tendons through an approximately 2 cm fibro-osseous tunnel along the radial styloid. A septum often separates the two subcompartments – this knowledge results in reduced pain and must be considered during injection procedures and operative treatment. Ultrasonography-guided injection targeting both subcompartments has resulted in documented improvement in success rate. (StatPearls, 2023).
Common Causes and Risk Factors — Why Tendon Sheaths Become Inflamed
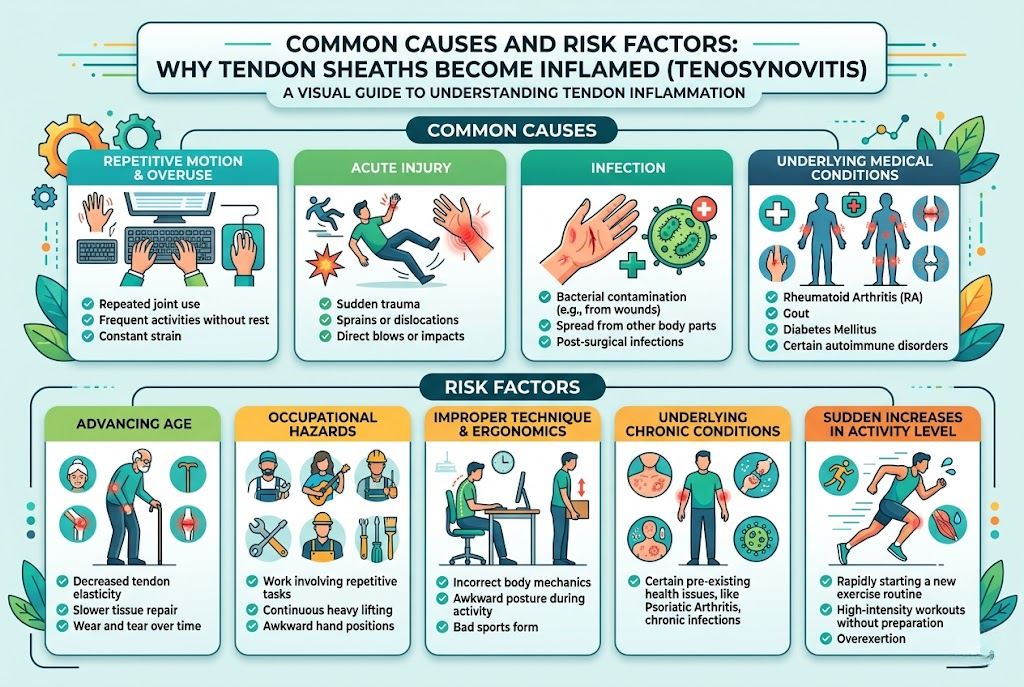
Repeated repetitive motion, biological susceptibility, or in rare instances, infectious injection leads to five main causes of tenosynovitis that each require unique treatment.
What Is the Cause of Tenosynovitis?
Repetitive strain injury is the most common cause of the condition, in which case a single movement like the use of a computer mouse is repetitively performed hundreds or thousands of times on a daily basis, and over days, weeks, years can result in inflammation. This occurs in assembly line workers, artists, women who repeatedly do hair-titching, and millions of new mothers. Long hours on a cell phone text messaging are attributable to the condition.
Pregnancy and the postpartum period constitute significant hormonal risk factors. Increased fluid retention in late pregnancy can increase pressure within the tendon sheath, while repetitive breastfeeding and infant handling further exacerbate the mechanical stress. The process is usually resolved once the hiatus between patients’ hands, wrists, and shoulders occurs with frequency.
Infectious Tenosynovitis occurs when microorganisms – most frequently S. aureus – invade the tendon sheath through either a puncture wound, animal bite, or (becoming increasingly rare) surgical site. Infectious tenosynovitis constitutes a true surgical emergency – failure to rapidly identify and eradicate the offending infectious agent (by antibiotics and the operating room) risks tendon necrosis and even amputation in the most dire circumstances. Patients with immune suppression and diabetes are much more susceptible to infectious tenosynovitis and tend to have worse outcomes.
Autoimmune conditions (including reactive arthritis, gout, and psoriasis) induce systemic immune dysregulation that can lead to inflammatory tenosynovitis without necessarily subjecting the tendons to mechanical stress. Chronically dysregulated immune attack on synovial membrane results in progressive damage to the underlying tendons and fibrosis of the sheath.
💡 Common Misconception
Many patients feel fatigued if the sit at a computer for a few hours, but it turns out thev’e never had trouble typing through a carpal tunnel or radiocarpal syndrome attack. Office workers, creatives, musicians, and even so-called “weekend warriors” are susceptible to the same tendinoses that afflict construction crews or industrial laborers. In overuse injury, a tennis elbow (lateral epicondylitis) pattern of injury can appear in the wrist during long periods of keyboard and mouse use.
Symptoms and Diagnosis — How Doctors Identify Tenosynovitis
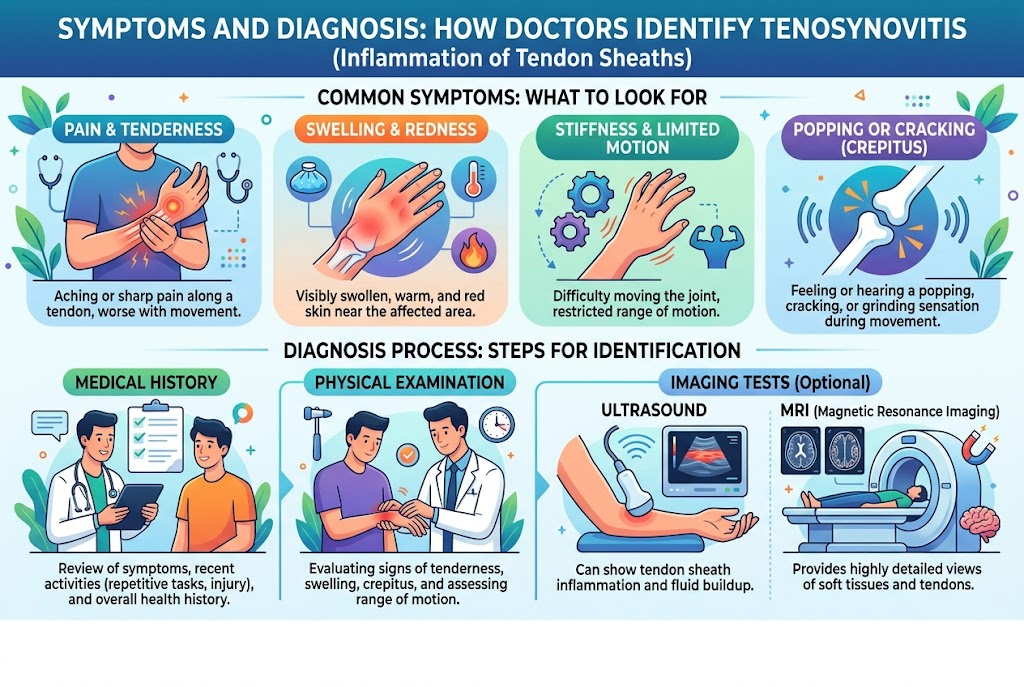
Common presenting complaints to primary care are pain and swelling along the course of the affected tendon and its sheath, altered joint mobility, and potentially crepitation of the involved tendon with tactile mobility. Pain following activity and its alleviation with rest is an expected experience. Specific to de Quervain’s tenosynovitis, patients often report pain to the radial side of their wrist that escalates when gripping, twisting, or contorting the hand into a fist.
How Is Tenosynovitis Diagnosed?
Following a thorough physical exam and history taking, clinicians with a high suspicion of de Quervain’s tenosynovitis administer either the Finkelstein or related Eichhoff maneuver to elicit pain and determine diagnosis. During the Finkelstein maneuver, the patient places the thumb in palmar flexion and then the examiner tilts the hand ulnarly (away from the thumb). The test is positive if the maneuver causes pain along the course of the radial styloid. The alternate Eichhoff maneuver tasks the patient to contract their thumb into the palm of their hand and then tilt the hand ulnarly. False positives of the Eichhoff maneuver emerge in some wrist pathologies.
In patients where infectious flexor tenosynovitis is suspected, signs noted include the four cardinal Kanavel signs: (1) fusiform swelling of the entire finger, (2) a flexed posture of the fingers, (3) tenderness over the course of the flexor tendon sheath, and (4) severity of pain on passive extension of the finger. Data published by the JMA Journal (2024) notes that the Kanavel signs have a sensitivity in excess of 90%, but a specificity of about 50%.
⚠️ Emergency Warning — Infectious Tenosynovitis
If you have a fever and fusiform swelling of the entire finger along with pain severe enough to be aggravated when your finger is extended by someone else, you have an orthopedic emergency. Infectious flexor tenosynovitis can be life-threatening. If treatment is delayed beyond 24 hours, there is a 77% increased chance of permanent tendon damage; advanced cases risk amputation.
| Condition | Key Difference | Distinguishing Test |
|---|---|---|
| Tenosynovitis | Pain along tendon sheath; crepitus on movement | Finkelstein test (De Quervain’s); Kanavel signs (infectious) |
| Tendonitis | Pain at tendon insertion; no sheath involvement | Point tenderness at tendon-bone junction |
| Carpal Tunnel Syndrome | Numbness/tingling in median nerve distribution (thumb, index, middle finger) | Tinel’s sign; Phalen’s test; nerve conduction study |
| Thumb CMC Osteoarthritis | Bony enlargement at thumb base; grinding sensation | Grind test; X-ray showing joint space narrowing |
Imaging studies are not usually indicated for diagnosis of tenosynovitis. Ultrasound, however, can be a highly effective initial modality because it can demonstrate tenosynovial fluid collection, anatomical variations such as the septum within the first dorsal compartment, and can guide injections to appropriate sites of delivery. Magnetic resonance imaging (MRI) demonstrates the best soft tissue detail and is used when the diagnosis or severity are uncertain. X-ray findings are most helpful to exclude osteoarthrosis and fractures.
Tenosynovitis Treatment Options — De Quervain’s and Beyond

When deciding upon treatment for tenosynovitis the extent of presentation (acute versus chronic and degree of severity) and etiology (infectious versus non-infectious) must be taken into consideration. Most patients with non-infectious tenosynovitis are initially treated with conservative measures and transition to injections or surgery only when these methods fail. On the other hand, infectious tenosynovitis is marked by a rapid progression to surgical intervention.
Conservative Management
Initial management of non-infectious tenosynovitis consists of rest, behavioral modifications (for example, avoiding repetitive manipulations of the inflamed area), and immobilization with a wrist splint or brace. For de Quervain’s tenosynovitis, the appropriate splint is a thumb spica, which confines motion to the thumb and wrist and allows inflammation resolution. Oral NSAIDs such as 400-600 mg of ibuprofen or 250-500 mg of naproxen, dosed every 6-8 hours or twice daily respectively, provide antiinflammatory and analgesic relief, helping to reduce inflammation and pain.
An all-too familiar story: a graphic designer develops wrist pain after working intensely for a month. She attempts various stretching exercises, swaps her mouse, and applies ice to the problem area. After three painful weeks, switching mice alone gives her no symptom improvement. When she gets on-board with a thumb spica splint, two consecutive weeks of complete rest from computer mouse use, and naproxen, the inflamed tissues begin to settle. The takeaway? Inadequate rest doesn’t work; at some point inflammation needs to fully resolve.
Corticosteroid Injections
When symptoms persist for 4-6 weeks despite conservative therapy, corticosteroid injections are recommended. A review published in StatPearls (2023) found corticosteroid injections provided almost complete relief in 52-90% of patients with de Quervain’s following one or two injections, respectively. One prospective study corroborates corticosteroids efficacy with a 73.4% success rate.
A 2024 systematic review published in the Journal of the American Medical Association Network Open supports corticosteroid injections plus thumb spica immobilization for 3-4 weeks as the best first-line treatment.
However, recurrence is still a major issue. A recent study published in the Journal of Personalized Medicine (2024) demonstrates a 30% recurrence rate with corticosteroid injection with significant improvement on the DASH disability scale. A study published at the 2026 Hand Surgery Meeting shows that following first injection, 6.69% go to surgery and 26.8% get repeat injections.
💡 Pro Tip — Ice or Heat for De Quervain’s?
During the acute inflammatory (first 2-3 weeks) stage then, ice for 15-20 minutes several times a day in order to prevent the formation of edema. Once the acute inflammatory phase has finished, heat packs may be beneficial but applied several minutes to warm up the tissue before moderate pain free exercise. The majority of patients find they can be confused when to switch over but simply if the area still appears swollen or warm then cold should be used, if the swelling has subsided then heat may be applied prior to gentle movement.
Infectious Tenosynovitis Treatment
Infective flexor tenosynovitisis an orthopedic emergency that demands a totally different treatment plan. Managed with intravenous broad spectrum antibiotic therapy (staph/staph covered often) and surgical decompression as necessary. Referring to Michon classification as follow: Stage 1 (serous exudate) may be treated by catheter irrigation, stage 2 (purulent exudate) treated with minimally invasive decompression and stage 3 (tendon necrosis/ sheath) requires open debridement and amputation
Immunocompromised patients and diabetics are a different case. Early surgical treatment without waiting for antibiotic response is the rule for these patients. If medical treatment alone is decided patients need inpatient observation for a minimum of 48 hours.
In the absence of a clear response at 12-24 hours surgical drainage has to be performed.
Surgical Treatment
Surgical management is possible if treatment (conservative and two corticosteroid injection) is ineffective in providing lasting relief. Surgery for de Quervain’s release involves a small incision (around 2 cm) over the first dorsal compartment and incising of the tendon sheath to decompress the tendons. This is usually performed in clinic with local anesthetic and is a successful procedure in most series (> 90%).
In trigger finger (stenosing tenosynovitis), surgical release of the A1 pulley has also been shown to have success rates greater than 90%. Surgical complications are rarely reported and include superficial radial nerve injury, tendon subluxation and hypertrophic scarring.
DMARDs for Autoimmune-Driven Cases
Tenosynovitis caused by an underlying autoimmune problem such as rheumatoid arthritis, inflammatory arthritis or gout..would generally require systemic disease-modifying antirheumatic drugs (DMARDs) along with local treatment. To attain the underlying disease, medications like methotrexate, hydroxychloroquine and new biological drugs are used rather than the local treatment.
Emerging Therapy — Platelet-Rich Plasma (PRP)
A recent study comparing platelet rich plasma (PRP) injection with corticosteroid injection in de Quervain’s tenosynovitis showed the corticosteroid group had significantly superior results at 2 weeks, but the PRP group significantly out performed by 6 months. Both procedures were demonstrated to be safe. PRP is a new option in the treatment of de Quervain’s that can reduce pain over the long term, avoiding the tendon weakness after multiple corticosteroid injections, although guidelines are not yet established.
The 4-6-2 Protocol — A Treatment Decision Framework
One approach uses in a stepwise fashion by which the patient and clinician can go through the escalation of treatment for non-infectious tenosynovitis:
- Weeks 0-4: Conservative management — NSAIDs and splinting, rest, activity modifications. Follow-up at 4 weeks.
- Weeks 4-6: No significant improvement: corticosteroid injections into the tendon sheath (ultrasound-guided if available).
- Failed injections 2x: referral to a hand surgeon for surgical release discussion.
Exception: infectious tenosynovitis follows immediately after under going the conservative management plan. Seek emergency care. Autoimmune presentation requires concurrent rheumatology referral and systemic disease modifying anti-rheumatic drugs (DMARDs).
| Treatment | Success Rate | Timeline | Recurrence | Invasiveness |
|---|---|---|---|---|
| Rest + Splint + NSAIDs | Varies (mild cases) | 4–6 weeks | High if activity resumes | None |
| Corticosteroid Injection | 52–90% | Days to weeks | ~30% | Minimal (needle) |
| PRP Injection | Comparable to steroid (better at 6 months) | 2–6 months | Lower than steroid (preliminary data) | Minimal (needle + blood draw) |
| Surgical Release | >90% | 6–12 weeks full recovery | Low | Outpatient surgery |
| IV Antibiotics + Drainage (Infectious) | Depends on stage (Michon I-III) | Days to weeks (inpatient) | Low with prompt treatment | Moderate to high |
“In my clinical experience, the patients who struggle most with tenosynovitis recovery are those who return to the aggravating activity too soon after injection. A corticosteroid shot reduces inflammation quickly, but the underlying mechanical problem remains. Without genuine activity modification, the sheath re-inflames within weeks.”
— Dr. Christopher S. Crowe, MD, Hand and Upper Extremity Surgery, Stanford University
Exercises and Rehabilitation — Restoring Mobility and Strength

Rehabilitation is perhaps the most overlooked aspect of tenosynovitis treatment found in most online resources. Research established the benefit of structured exercise programs- specifically tendon gliding exercises- when implemented at the appropriate time. From broad clinical research combined with extensive amounts of patient anecdotes, it has become clear that the commonality in successful recovery is taking the time to require the appropriate physiological rest period prior to active rehabilitation instead of pushing through the acute inflammatory phase prematurely.
Endless anecdotes of this principle emerges in online forums like r/DeQuervains: “Physical therapy generally will make it worse pre-op but can be helpful for post-op recovery”, or “I avoided doing any exercises that caused pain, even if it was just a bit, and it was going away in about two months” all note the same idea recognized in clinical practice: slow rehabilitation prevents reinitiation of the inflammatory phase.
| Phase | Timeframe | Exercises | Frequency |
|---|---|---|---|
| Phase 1 — Acute (Rest) | Weeks 1–2 | Gentle active range of motion exercises; tendon gliding exercises (make a fist → straighten → hook fist → tabletop → full fist); avoid all pain-provoking activities | 3× daily, 10 repetitions each |
| Phase 2 — Recovery | Weeks 3–4 | Progressive grip strengthening (squeeze therapy putty); wrist flexion/extension with light resistance; thumb opposition exercises | 2× daily, 2 sets of 10 |
| Phase 3 — Return | Weeks 5–8 | Functional and occupation-specific exercises; gradual return to full activity; eccentric wrist exercises for long-term tendon health | Daily, integrated into routine |
Complementary Approaches
Treatment of complementary modalities continue to find evidence through clinical trials. Results from the 2022 randomized controlled trial by Leung et al. determined that acupuncture ‘risk-free and effective’ in alleviating pain intensity and increasing grip strength in tenosynovitis. A 2024 systematic review and meta-analysis also recognized that acupuncture “displays a promising trend of relieving tenosynovitis pain”.
For those patients who wish to explore TCM treatment options for tenosynovitis — including acupuncture, tuina therapeutic massage, and moxibustion — these can be used as adjuncts for pain management. Cupping therapy (hijama) can be considered as well by some patients in alleviating local swelling.
Consultation with an occupational therapist is appropriate for splinting tips, ergonomic work station assessments, and progression of suggested exercise regimens tailored to your particular work lifestyle. This position is more pertinent to those who work in increased ergonomic risk environments that relate to work-specific tenosynovitis.
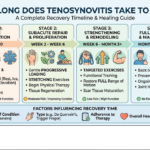
Recovery Timeline and Prevention — Long-Term Tendon Health

Recovery time from tenosynovitis greatly depends on approaches taken. Knowing expected timelines leads us to avoid two known mistakes- removal of conservative treatment is prematurely because we don’t see rapid results, and rushing back to normal activities prior to fiber layer healing.
Recovery Timelines by Treatment Type
- Conservative (rest + splint + NSAIDs): 4-6 weeks for symptom resolution in mild-to-moderate cases
- After corticosteroid injection: Symptoms begin to improve within a few days, with maximum benefit in 2-3 weeks. Patients treated with cortisone injections may take 3-9 months to recover completely.
- After surgery (De Quervain’s release) suture removal at ~2 weeks, resume limited activity at 2-4 week, full recovery at 6-12 weeks
- Infectious tenosynovitis: Variable – based on severity of infection (Michon stage) and health status of patient; prolonged recovery for elderly and diabetic patients
One of the most common errors patients make is abandoning rehabilitative exercises when pain subsides. Many tenosynovitis patients have posted on various online forums about how exhausting the study of tender tendons can be; relief of pain after an injection or rest leads to a gradual return to full activity only to have the pain recur weeks later. Continued gentle tendon gliding exercises and ergonomic interventions posttreatment to avoid recurrence is important.
Workplace Ergonomic Prevention
- ✔
Keyboard and mouse positioning: Keep wrists in a neutral position (not bent upward or to the side). Consider a vertical mouse or ergonomic keyboard to reduce wrist deviation. - ✔
Micro-breaks every 30 minutes: Set a timer. Perform 30 seconds of tendon gliding exercises and wrist circles during each break. - ✔
Tool grip modification: Use tools with padded, larger-diameter handles to reduce grip force. Avoid prolonged pinching motions. - ✔
Workstation assessment: Request a formal ergonomic evaluation from your employer — many companies provide this service. Focus on monitor height, chair armrest position, and desk height. - ✔
For musicians and athletes: Warm up before playing. Gradually increase practice duration. Build rest days into training schedules. A related condition — knee pain from overuse — follows similar prevention principles.
💡 Key Takeaway
Tenosynovitis is well-defined as a self limiting. When initial treatment is administered quickly, coupled with a true adaptation of activity, then the condition usually resolves. The patients who suffer chronic or repeated episodes are the ones who go back to activity ‘too soon’.
Consider tendon sheaths like a blister – even when the pain subsides, the tissue requires extra time to redevelop structure.
Frequently Asked Questions
Q: What is the best treatment for tenosynovitis?
View Answer
Treatment varies according to etiology. The initial management of most non-infectious tenosynovitis is Rest, splintage, NSAIDs and modification of activity. Patients not responding to conservative management in 4-6 weeks can be offered corticosteroid injections with a success rate of 52-90%.
Infectious tenosynovitis requires urgent IV antibiotics as well as possible surgical drainage.
Q: How long does tenosynovitis take to heal?
View Answer
Range from 4 weeks to several months. Mild conservatively managed cases improve within 4-6 weeks. Post-injection recovery is from a few days up to weeks for initial improvement, with resolution taking 3-9 months.
Surgical recovery of 6-12 weeks for full return.
Q: Does tenosynovitis go away on its own?
View Answer
De Quervain’s tenosynovitis may be self-limiting and resolve spontaneously—this is often seen post-partum, as the symptoms traditionally resolve when the lifting stress has abated, but in the majority of cases rest and modification of activities is enough. Without intervention, chronic cases are prone to the complications of adhesions and persistent stiffness.
Q: What happens if tenosynovitis goes untreated?
View Answer
Chronic pain, joint contracture, tendon adhesions (scarring), and ruptures of the tendon may all occur if tenosynovitis goes untreated. Of the types of tenosynovitis, the infectious variety has the greatest risks, since delays in treatment could result in potential tendon necrosis and finger amputation.
Q: Can tenosynovitis be prevented?
View Answer
Yes, in many instances. Some important prevention recommendations are frequent microbreaks in repetitive movements, neutral wrist position, ergonomic tools; bend and extend the tendons (tendon gliding) as part of warm-up. Formal workstation assessment should be provided in the occupational setting.
Q: How do you fix tenosynovitis?
View Answer
Treatment is stepwise: rest and splinting for 4 weeks, then corticosteroid injection if symptoms persist; if after two injections symptoms remain, surgical release should be considered. Underlying cause, whether repetitive motion, infection or autoimmune disease needs to be tackled for complete resolution. Rehabilitation exercises should be continued throughout even after symptoms improve to prevent recurrence.
Considering Complementary Treatment for Tenosynovitis?
Tong Ren Tang’s DHA-registered doctors of acupuncture, massage (tuina) and herbal medicine provide evidence-based complementary therapies to orthodox tenosynovitis treatment. Decades of pioneering clinical experience have shaped our Dubai clinic’s bespoke protocols.
Our Perspective on Tenosynovitis Care
This guide was reviewed by the Tong Ren Tang clinical team in Dubai, drawing on both peer-reviewed orthopedic research and our experience treating tendon and joint conditions with integrated Traditional Chinese Medicine approaches. We present all treatment options — conventional and complementary — because informed patients make better recovery decisions. Clinical data in this article references published studies from the NIH, JAMA, and leading orthopedic journals.
References & Sources
- De Quervain Tenosynovitis — StatPearls (Updated Nov 2023) — National Library of Medicine / NIH
- Effectiveness of Corticosteroid Injections for Treatment of de Quervain’s Tenosynovitis — PubMed Central / NIH
- Clinical Outcome of Nonoperative Treatment of de Quervain’s Disease — PubMed Central / NIH
- Management of de Quervain Tenosynovitis: A Systematic Review — JAMA Network Open
- De Quervain Tendinopathy: Anatomical Prognostic Indicators — Journal of Personalized Medicine (2024)
- Kanavel’s Signs and Pyogenic Flexor Tenosynovitis — PubMed Central / NIH
- Acupuncture for de Quervain’s Tenosynovitis: A Randomized Controlled Trial (Leung et al., 2022) — PubMed / NIH
- Systematic Review and Meta-Analysis of Acupuncture for De Quervain’s (2024) — PubMed / NIH