Get in Touch with Tongren Tang Gulf
Does acupuncture work? Yes – for certain conditions, the research is now clear enough that Federal health agencies and leading medical guidelines recommend it, and for others the research evidence is weak or nonexistent. An honest response balances sorting through what tens of thousands of patients in research trials actually tells us, including proven indications, still-contentious ones, and what science really can’t tell us about the benefits of acupuncture.
Quick Verdict
| Strong evidence for | Chronic low-back pain, knee osteoarthritis, post-op nausea |
| Moderate evidence for | Migraine prevention, tension headache, chemotherapy nausea, fibromyalgia |
| Weak / contested for | IVF success, smoking cessation, weight loss, hot flashes (vs sham) |
| Largest meta-analysis | Vickers 2018 — 39 trials, 20,827 patients, effects persist 1 year |
| Safety | Serious events rare in audits of nearly 200,000 patients; pneumothorax most reported |
The Short Answer: Where Acupuncture Works and Where It Doesn’t

Most authoritative evidence on the effect of acupuncture for chronic pain comes from a 2018 individual-patient-data meta-analysis of 39 randomized controlled trials involving 20,827 patients. Relative to no acupuncture, this treatment shows a moderate clinical trial effect size (roughly 0.5 SDs) in pain scores. Relative to sham acupuncture, where needles may be superficially and at non-specific points inserted, the effect is smaller (roughly 0.2 SDs). Both results are statistically significant, and the trial follow-up was for a full year with a modest 15% reduction in impact (Vickers et al., Journal of Pain, 2018). An interconnected series of 39 individual trials utilizing the most rigorous methodology confers uncommon weight to the conclusion for any used healthcare intervention.
Understanding that nuance is important. Acupuncture is not a placebo, but the low difference between real (vs sham) acupuncture is less of a difference than acupuncture and no intervention at all, indicating the role of the patient/clinician interaction, the ritual of treatment, and stimulus via the acupuncture needle itself. For particular conditions such as acupuncture for IVF success, acupuncture for smoking cessation, acupuncture for hot flashes, that low real-vs-sham gap isn’t even there. Studies on the efficacy of acupuncture for these specific indications consistently fail to show specific benefit.
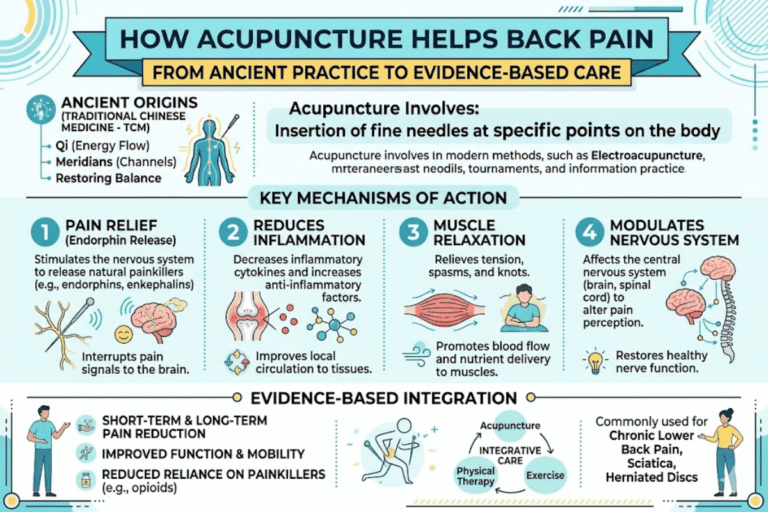
How Acupuncture Works: Two Frameworks That Don’t Always Agree
Tell a Chinese medicine practitioner and a Harvard neurologist how acupuncture works and both explanations will be internally coherent, yet neither has been shown to fully explain why using acupuncture produces measurable effects.
Classical TCM FrameworkIn Traditional Chinese Medicine, health is dependent on the uninterrupted flow of qi (energy) along defined pathways called meridians. Aetiologies are then identified and diagnosed clinically as qi obstructions, deficiency states, stagnation, and the like. Professionals perform diagnosis with tongue examination and pulse diagnosis at three points bilaterally, complemented by interpersonal investigation (Wu, 1978). Fine filiform needles stimulate specific acupoints along a network of channels to balance the qi flow.
Modern Neurophysiological FrameworkStimulation of A-delta fibers and C fibers activates brainstem-based inhibitory pathways and endogenous opioid release. Imaging studies have demonstrated that acupuncture analgesia maps to changes in pain-processing regions in the cortex and centers of the central nervous system. Physiological effects at the acupuncture insertion site have been observed through a biomechanical effect on collagen fibers in the fascial planes.
How does acupuncture work scientifically?
Mechanistically, the most defensible answer is that acupuncture has at least three overlapping effects- nervous-system effects (detailed in the animal and imaging literature cited above), tissue effects (on the connective tissue at the site of the needle), and large nonspecific effects from expectation, practitioner desire, and the ring of the ritual.
National Center for Complementary and Integrative Health health information clearly states that “how acupuncture works is not fully understood,” a very honest, if not exactly reassuring statement from a federal health agency, and one that Western medicine still does not want to acknowledge.
“Decreases in pain after acupuncture cannot be explained solely in terms of placebo effects. Variations in effect size are driven predominantly by differences in treatments received by the control group rather than by differences in the characteristics of acupuncture treatment itself.”
— Andrew J. Vickers and the Acupuncture Trialists’ Collaboration, Journal of Pain 2018
Conditions Acupuncture Helps (Sorted by Evidence Strength)

The following Evidence-Tier Framework classifies indications based on the strength of the systematic-review evidence rather than how frequently the conditions are marketed as “treatable with acupuncture.” References are cited adjacent to each row, so you can check the source of each tier.
| Condition | Tier | Evidence Snapshot |
|---|---|---|
| Chronic low-back pain | Strong | 12 studies, 8,003 patients; ACP 2017 first-line nondrug option; pain relief comparable to NSAIDs |
| Knee osteoarthritis | Strong | 10 studies, 2,413 patients; ACR/Arthritis Foundation 2019 conditional recommendation |
| Migraine prevention | Moderate | Cochrane 2016: 22 studies, ~5,000 patients; modestly better than sham; better dropout than drugs |
| Tension-type headache | Moderate | Cochrane 2016: 12 studies, ~2,350 patients; moderate-to-low quality |
| Post-operative pain | Moderate | 11 studies, 682 patients — less pain and lower opioid use one day post-op |
| Aromatase-inhibitor joint pain (breast cancer) | Moderate | JAMA 2018 RCT: 226 women, 6 weeks of acupuncture reduced joint pain |
| Chemotherapy / post-op nausea | Moderate | Long-standing expert consensus, though pre-current antiemetics |
| Fibromyalgia | Moderate | 12 studies, 824 patients; better than sham at low-to-moderate quality |
| Stress urinary incontinence | Moderate | JAMA 2017: 500 women, electroacupuncture; two-thirds achieved ≥50% leakage reduction |
| Hot flashes (menopause) | Weak | Better than no treatment, NOT better than sham acupuncture |
| IVF / infertility | Weak | 2021 review: 6 studies, 2,507 patients — no difference in pregnancy or live birth vs sham |
| Smoking cessation | Weak | Cochrane 2014: 9 studies, 1,892 patients — no significant 6-month benefit |
Strongest effects concentrate around musculoskeletal complaints — chronic low-back pain, knee OA, neck pain, and headache. Acupuncture appears to have reasonable evidence for a number of non-pain indications- allergic rhinitis, urinary incontinence, treatment-related nausea- and weak or no evidence for fertility, smoking cessation, weight loss, and many cosmetic claims.
What the Best Studies Actually Show (and Why They’re Hard to Run)

What makes acupuncture research difficult is creating a convincing placebo. You can give one group a sugar pill that appears identical to the real medication. In an acupuncture trial — particularly trials of acupuncture for chronic pain — you can’t mimic the needle very easily. Researchers have used retractable “sham” needles that touch the skin without puncturing, or inserting real needles at a nonmeridian point. Both of these options still results in some sensation, some practitioner attention, and some expectation in the patient-meaning the placebo condition is often a treatment in its own right.
This methodological issue is why the bulk of meta-analyses still show a real-vs-sham difference, just a lot smaller than the no-treatment-vs-acupuncture difference. American Pain Society’s conclusion based on the Vickers data is that acupuncture is “a reasonable option for a patient with chronic pain” – wary language, not a sales pitch. Acupuncture may not be a cure, but where evidence is strong, it is worth its place in pain management.
Is acupuncture better than placebo?
Yes, modestly. In the chronic pain conditions examined by Vickers, real acupuncture outperformed sham by an average of 0.2 standard deviations in pain scores- small but statistically significant. In select indications (hot flashes, IVF, carpal tunnel) the difference disappears. This honest interpretation: acupuncture has specific effects over placebo for chronic musculoskeletal pain and headache, but the difference varies by condition.
💡 How to spot a high-quality acupuncture study
Watch for: (1) sham control with credible blinding, (2) at least 100 patients per arm, (3) course of treatment of 6-8 sessions or more, (4) outcome months after the conclusion of the treatment course-not just at the last needle. Studies that examine only a single session of treatment are not informative.
What Happens at an Acupuncture Session (And What It Feels Like)

Most first visits take about an hour. The acupuncturist will ask about your presenting symptoms, habits and use of medication. The practitioner will examine your tongue, its shape and coating, your face color and the pulse felt at three points on each wrist. Because TCM diagnosis is based upon patterns rather than specific diseases, the intake process is somewhat more detailed than for most practitioners.
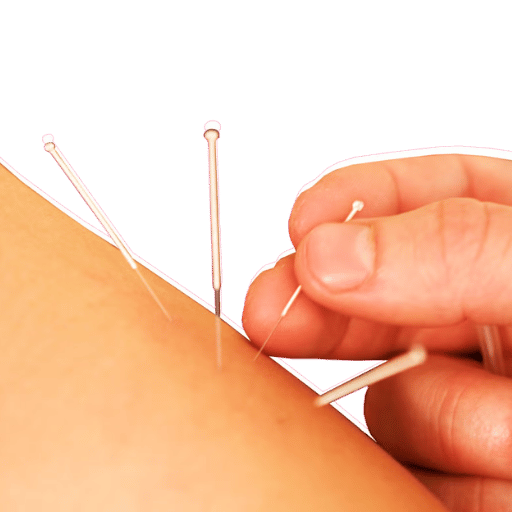
The therapy requires 5 to 20 disposable sterile acupuncture needles at a time, at precise locations. Insertion is usually painless – the needles are extremely fine. These thin needles are about the diameter of a human hair. Once the practitioner feels the needle has reached the appropriate depth, the patient may feel what’s known as a “de qi” sensation: tingling, numbness, heaviness, soreness, pressure. In traditional Chinese medicine, that sensation indicates that the physician has accessed the correct location, where thin needles into the skin are believed to engage the meridian most fully.
The needles will need to stay in for 10-20 minutes while the person remains, ideally, very still. Some practitioners move the needles about, and in some cases the needles will have small electrical impulses applied (electroacupuncture). When removed the person will typically feel either very relaxed, energized, or nothing at all.
How often should you get acupuncture?
Part of a typical chronic pain course would be one or two visits per week for 6-8 weeks. If a person has not shown improvement after roughly 6 visits the chances of improvement decline rapidly and most practitioners would suggest change or cessation of treatment. For an acute condition 1-3 visits are likely to suffice. For some conditions, like post stroke or for fertility, ongoing visits 4-8 weekly are often used.
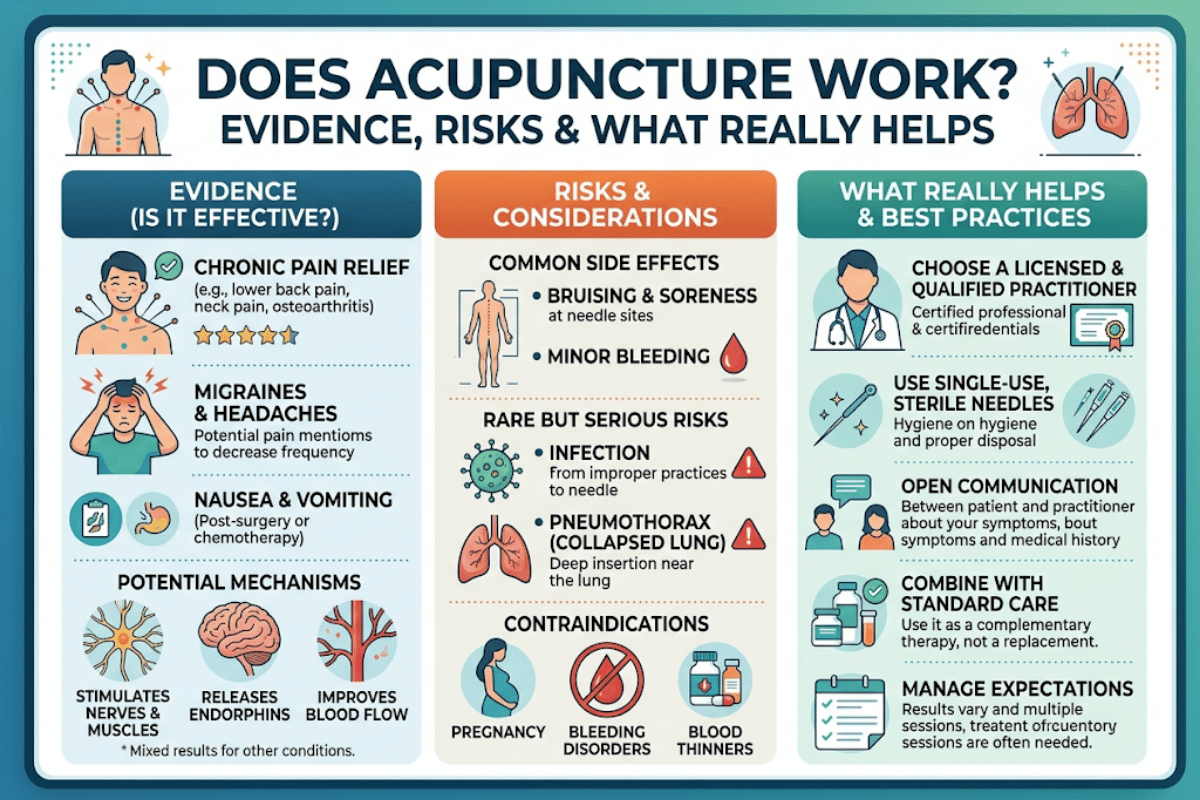
Safety, Side Effects, and Choosing a Qualified Acupuncturist

Acupuncture is a safe therapy when used by trained and accredited practitioners with sterile needles – which are actively monitored as Class II devices by the FDA in the United States. Its side effects tend to be minimal and brief lasting: mild bruising, pin point bleeding at needle site, brief dizziness; there have been no serious side effects noted for nearly 200 000 patients observed in prospective audits. The most common adverse event of significence may be the pneumothorax (partially collapsed lung due to overdeep needling) that has been recorded.
⚠️ Important contraindications
If you have a pacemaker, bleeding problems, are pregnant, have allergies to metals, are immunosuppressed, or are taking blood thinners notify the acupuncturist.
- ✔
Check that acupuncturist is licensed by your state – the majority of states now require non medical doctor practitioners to have NCCAOM certification - ✔
Make sure that electrical as well as regular needles are cleared for single use, having been cleared by the Food and Drug Administration - ✔
Find out how many patients with your problem they see – generalists are OK for many types of pain; specialists matter for fertility, post stroke - ✔
Disregard the popular (and unsubstantiated) idea of five banned points: there is no real classical list of universally deadly points, only increased risks associated with needling too deeply near the Bowels and other structures
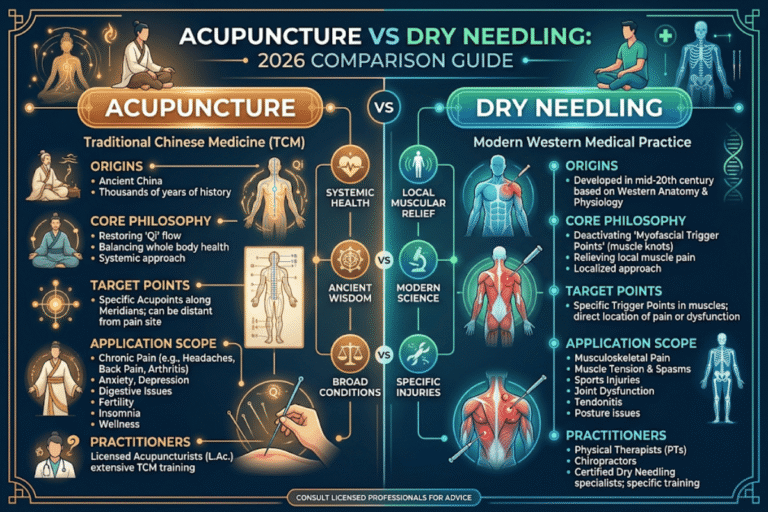
Acupuncture vs. Dry Needling: Why the Difference Matters
Another common question people have is whether acupuncture is the same as dry needling, which, despite use of similar needles, is based upon very different principles and tissue targets.
| Dimension | Acupuncture (LAc) | Dry Needling (PT/DPT) |
|---|---|---|
| Theoretical framework | TCM meridian / qi-flow | Western neuromuscular / trigger points |
| Target tissue | Acupuncture points along meridians (≈365 classical loci) | Myofascial trigger points (taut bands within muscle) |
| Practitioner training | ~3-4 year masters, ~1,900+ clinical hours, NCCAOM exam | Often a weekend course (~24-50 hours) on top of PT degree |
| Treatment indication | Broad: pain, nausea, allergies, headache, more | Narrow: musculoskeletal pain, especially myofascial |
| Best evidence base | Chronic pain meta-analyses (20,827 patients) | Trigger-point pain RCTs; smaller body of evidence overall |
Bottom line: if there is a specific muscle problem a physical therapist can help you with, dry needling might be an option. For more general chronic pain pictures, headache, nausea, allergic rhinitis – or for someone you want to have studied the full TCM diagnostic system – acupuncture is probably the better-trained pathway.
Types of Acupuncture: From Manual to Battlefield Protocols

“Acupuncture” is a blanket term for several distinct styles with different needling techniques and points.
- Manual acupuncture, the classical technique: a practitioner inserts and manipulates tiny needles at various body points. Most evidence-based published studies use this style.
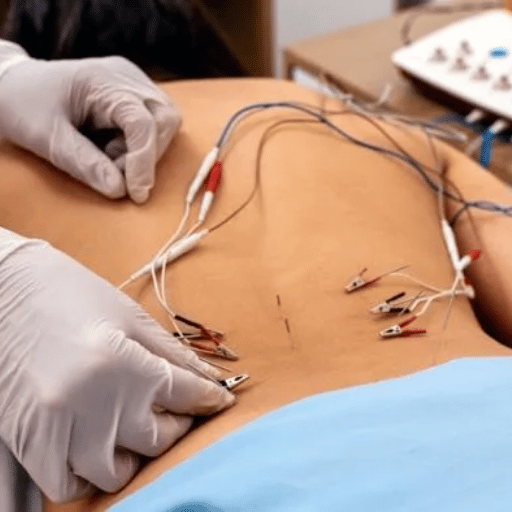
- Electroacupuncture is manual needles with electrical current running between them. It’s indicated for pain, nausea, stress urinary incontinence; the JAMA 2017 incontinence trial used 18 sessions of electroacupuncture.
- Auricular acupuncture (also called ear acupuncture) involves needle insertion or placement of beads at points on the outer ear. Has decent evidence for ongoing back pain and cancer pain in 2019-2020 reviews.
- Battlefield Acupuncture (BFA) is a 5-point ear protocol developed by the U.S. Department of Defense and adopted by Veterans Affairs facilities for rapid pain relief.
- Scalp acupuncture direct to points on the scalp, sometimes used in stroke rehab and neurological conditions.
- Cosmetic and facial acupuncture is marketed for skin tone and fine lines. Evidence base remains very weak and mostly in promotional forms rather than RCT reporting.
⚠️ The Battlefield Acupuncture paradox
Despite wide front-line adoption by the DoD and VA, a 2021 systematic review of 9 BFA trials of 692 subjects (Yang et al, American Journal of Chinese Medicine) showed no even trend of improvement over no treatment, usual care, sham BFA. Federal adoption is not the same as tested and confirmed efficacy – a good reminder how popular momentum can sometimes run ahead of the science.
Cost, Insurance, and Whether Medicare Covers It

A typical cash-only acupuncture visit in the US costs about $75 to $200, with the initial visit costing more because it includes a longer intake. Community acupuncture clinics who see several patients in one room will offer sliding-scale rates as low as $20 to $50 a visit.
Most people aren’t aware just how long a course of treatment adds up: 6-8 visits added together takes several hundred dollars, even without insurance reimbursements.
Insurance coverage has expanded over time, but is patchy. Among acupuncturist visits with some form of insurance coverage, the share rose from 41.1% in 2010-11 to 50.2% in 2018-19 (data from the Medical Expenditure Panel Survey). Medicare started to cover acupuncture on for chronic low-back pain in 2020- up to 12 visits, with another 8 covered if the first 12 produce noticeable improvement (CMS CAG-00452N). Medicaid coverage varies by state, and private coverage often only covers certain diagnoses like for chronic pain or chemo-related nausea. Always double check before making an appointment.
Where Acupuncture Research Is Heading

Several lines of work are reshaping the conversation:
- Research is converging around fascia as a mechanistic basis of some points of acupuncture. Director of the NCCIH Helene Langevin’s 2021 article in Life about fascia flexibility and use in myofascial pain has brought renewed interest in this area, beside the older neural-gate-control mechanism.
- Coverage continues to grow. Medicare’s 2020 decision on chronic low-back pain proved to be the most significant coverage shift in decades of U.S. coverage; even more expansion is probable if cost-effectiveness data are favorable.
- Federal coverage is being scrutinized. Systematic reviews can — and should — reevaluate frequently-used protocols, just as the Battlefield Acupuncture account provides an example of. Expect more such reviews, as the VA system accumulates outcome data.
- Use of acupuncture in the US is climbing. Adult U.S. acupuncture use went from 1.0% in 2002 to 2.2% in 2022, according to National Health Interview Survey information, published in JAMA.
If in 2026 you are contemplating acupuncture for chronic pain, consider whether your practitioner’s protocol is appropriate to provide evidence-strength (which is highest) and whether the practitioner can explain how six sessions with no progress should lead to termination.
When Acupuncture Is Worth Trying — A Decision Checklist
Try acupuncture if:
- You suffer from chronic pain 12 weeks or more past onset (knee, back, neck, fibromyalgia, headache)
- Standard treatments are insufficient or contraindicated
- You are able to dedicate to 6-8 appoints prior to evaluating results
- You can access an NCCAOM-certified or state-licensed practitioner
- Your expectations have been normalized: about half of S.D. enhancement can be achieved, but it is not a “cure”
Reconsider if:
- Your health problem is registered in the Weak-evidence tier (IVF, hot flashes, smoking cessation, weight loss vs sham)
- You have a pacemaker, bleeding disorder, or are immunocompromised
- You are pregnant; the provider is not specifically competent in point selection when pregnant.
- You believe the first appointment will resolve your problem most of the time – most courses include six to 12 treatments
Frequently Asked Questions
Q: Does acupuncture actually do something, or is it just placebo?
View Answer
It has a specific effect on chronic musculoskeletal pain and headache that goes beyond placebo – but the difference between real sham and real acupuncture is less than the difference between any two treatments: both effects exist.
Q: What conditions does acupuncture treat best?
View Answer
Chronic low-back pain and knee osteoarthritis have the most evidence backing. Fibromyalgia, tension headache, migraine prevention, post-operative pain, allergic rhinitis, and chemo-associated nausea exhibit moderate studies. Please reference the Evidence-Tier table above for greater detail.
Q: Is acupuncture covered by insurance?
View Answer
Coverage has increased – attending U.S. acupuncturists receive some reimbursement for about fifty percent of visits. Medicare covers chronic low-back pain (for a limit of 12 appointments since 2020). Medicaid and private insurance has different criteria depending on the plan and state of residence. Make sure your diagnosis qualifies prior to scheduling your series.
Q: Does acupuncture hurt? What does it feel like?
View Answer
Needle insertion is where the needles are most likely to be painless: they are the size of a human hair. When the practitioner has reached just the right depth, she may stimulate “de qi” – which may be experienced as a dull ache, pressure, numbness, heaviness, or tingling. This is not due to injury, and is believed to be the correct sensation.
Q: Can acupuncture help with anxiety?
View Answer
In a 2018 analysis of 64 depression investigations (7,104 patients), there was a moderate reduction in symptom severity versus “treatment as usual,” but most of these studies were of poor quality. There is less evidence collection specifically about anxiety. It can be a helpful adjunct to, but not replacement for, traditional treatment.
Q: How long does acupuncture take to work?
View Answer
Headache and joint pain due to musculoskeletal issues (knee, neck, back) are often receptive to 1 to 3 visits. Chronic pain generally requires 6 to 8 weekly appointments; in the Vickers analysis, effects lasted up to a year with only about a 15% decrease in effect toward the end. If no results have been realized by the completion of the 6th session, the chance of success diminishes greatly.
Tong Ren Tang’s Editorial Stance on This Article
Tong Ren Tang has looked after traditional Chinese medicine since 1669, having been supplying to the Qing’s imperial families for 188 years. The point is that we are not an acupuncture provider: we are a herbal-medicine pharmacy – but acupuncture is part of the TCM tradition that we are here to protect and preserve. This article has been composed to the same criteria as is applied to herbal remedies: don’t short change on quality.
This involves honest assessment of the acupuncture where the evidence is not strong.
References & Sources
- Acupuncture: Effectiveness and Safety — National Center for Complementary and Integrative Health (NCCIH), 2022 update
- Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis — Vickers et al., The Journal of Pain, 2018
- De Qi Sensation — NCI Dictionary of Cancer Terms — National Cancer Institute
- Acupuncture — Mayo Clinic — Mayo Foundation for Medical Education and Research
- Noninvasive treatments for low-back pain: a clinical practice guideline — Qaseem et al., American College of Physicians, Annals of Internal Medicine, 2017
- Acupuncture vs sham acupuncture or waitlist control on joint pain in breast cancer — Hershman et al., JAMA, 2018
- Acupuncture for the prevention of episodic migraine — Linde et al., Cochrane Database of Systematic Reviews, 2016
- Decision Memo for Acupuncture for Chronic Low Back Pain (CAG-00452N) — Centers for Medicare & Medicaid Services